25 years of experience in knee
Dr.Tsoukas has more than 25 years of experience in knee and arthroscopic surgery. He is one of the Knee Gurus globally
Anterior Cruciate Ligament( ACL) Rupture . Revision ACL
Dr. Tsoukas performed his first Anterior Cruciate Ligament Rupture Reconstruction in November 1999! The patient (A.D.) was a basketball player who played successfully after the operation for 20 years in high level, in Greece and abroad. He is still a very good friend with Dr. Tsoukas.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anterior Cruciate Ligament(ACL) Rupture . Revision ACL
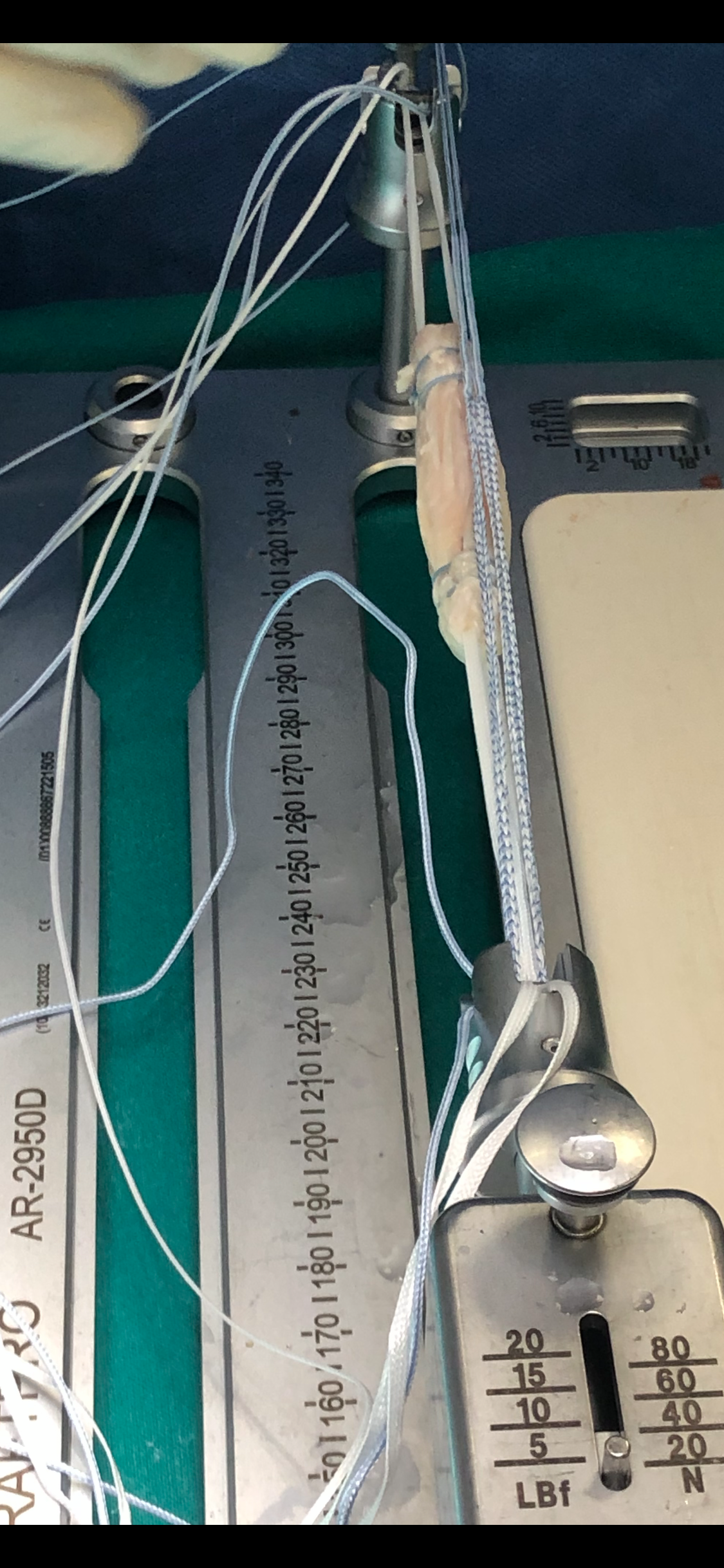
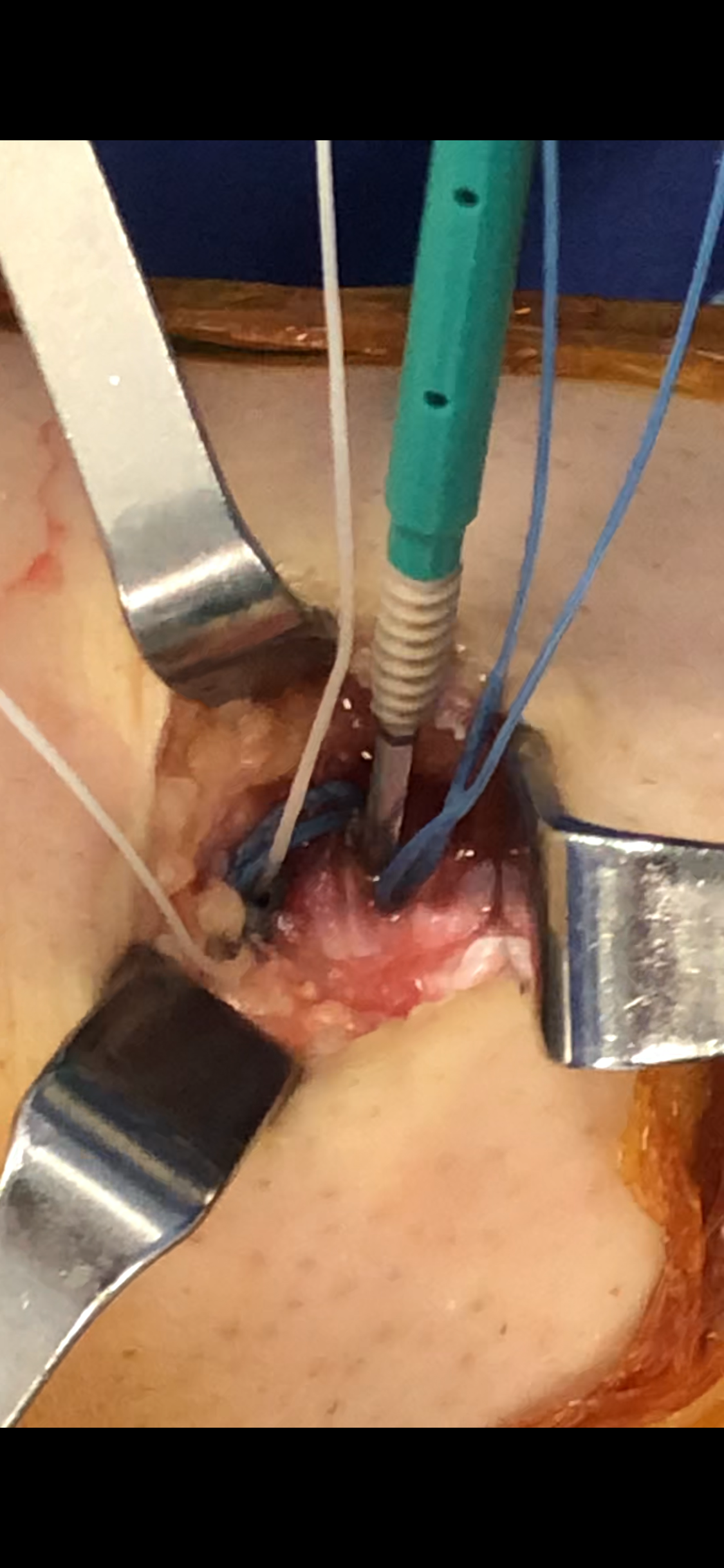
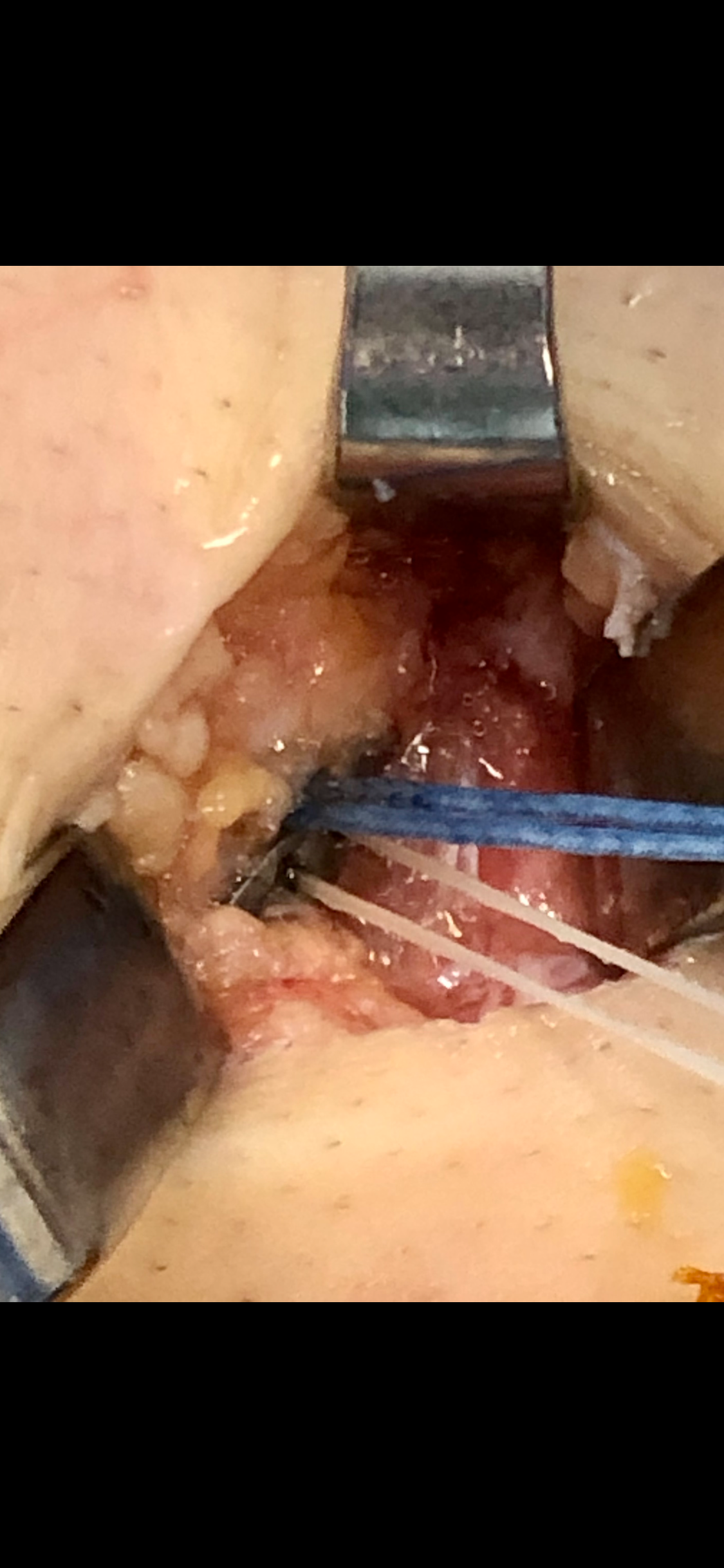
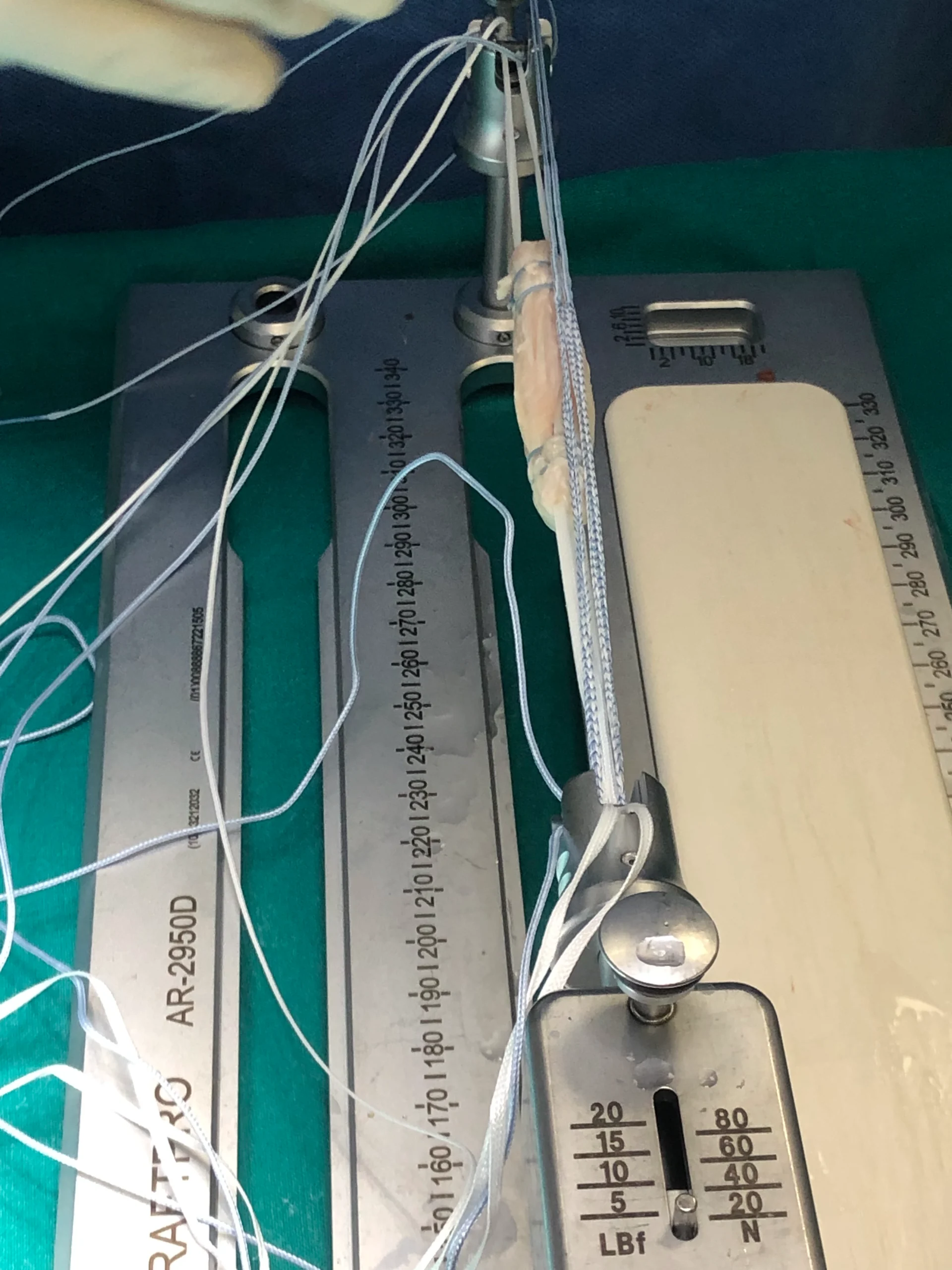
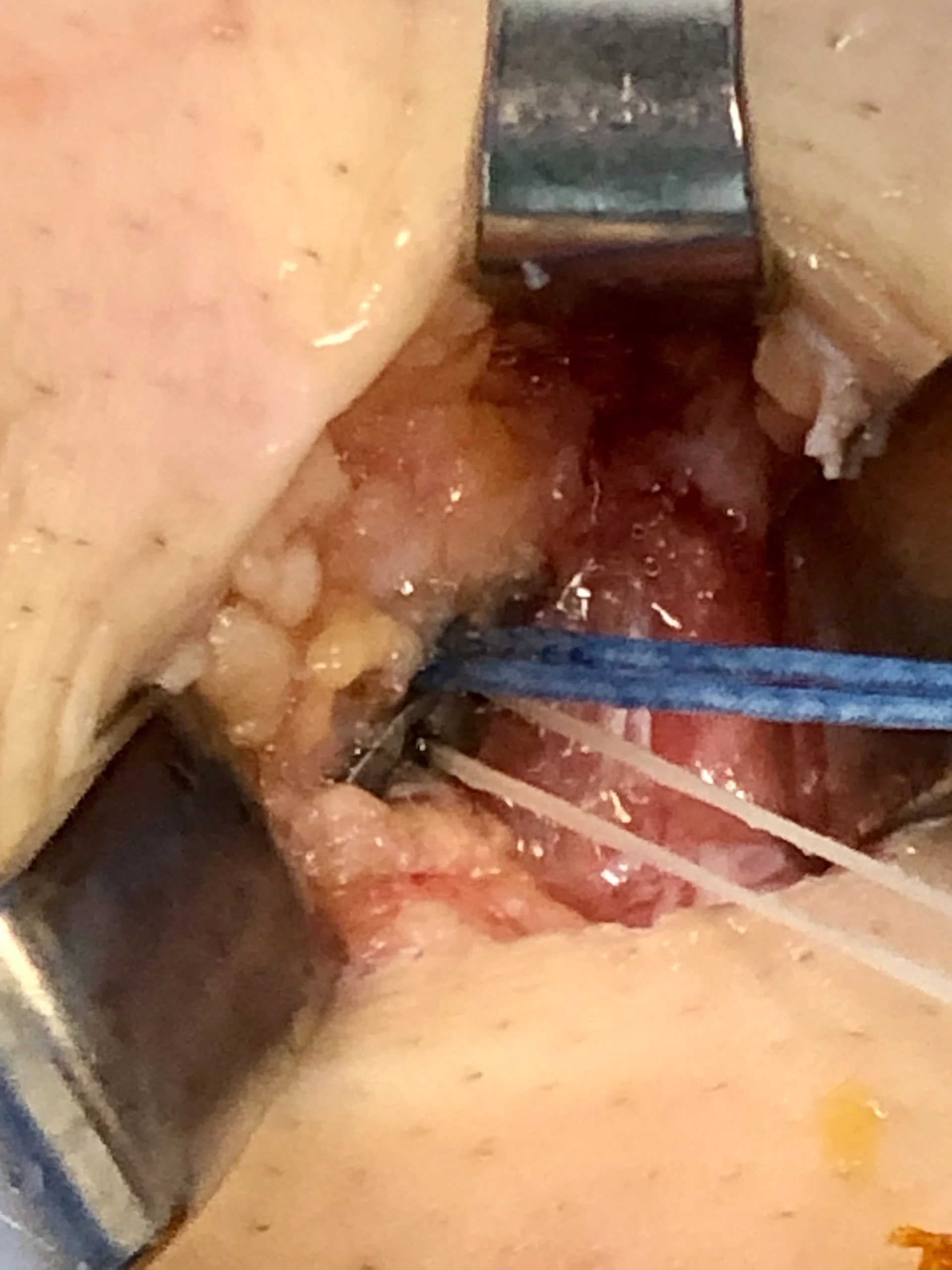
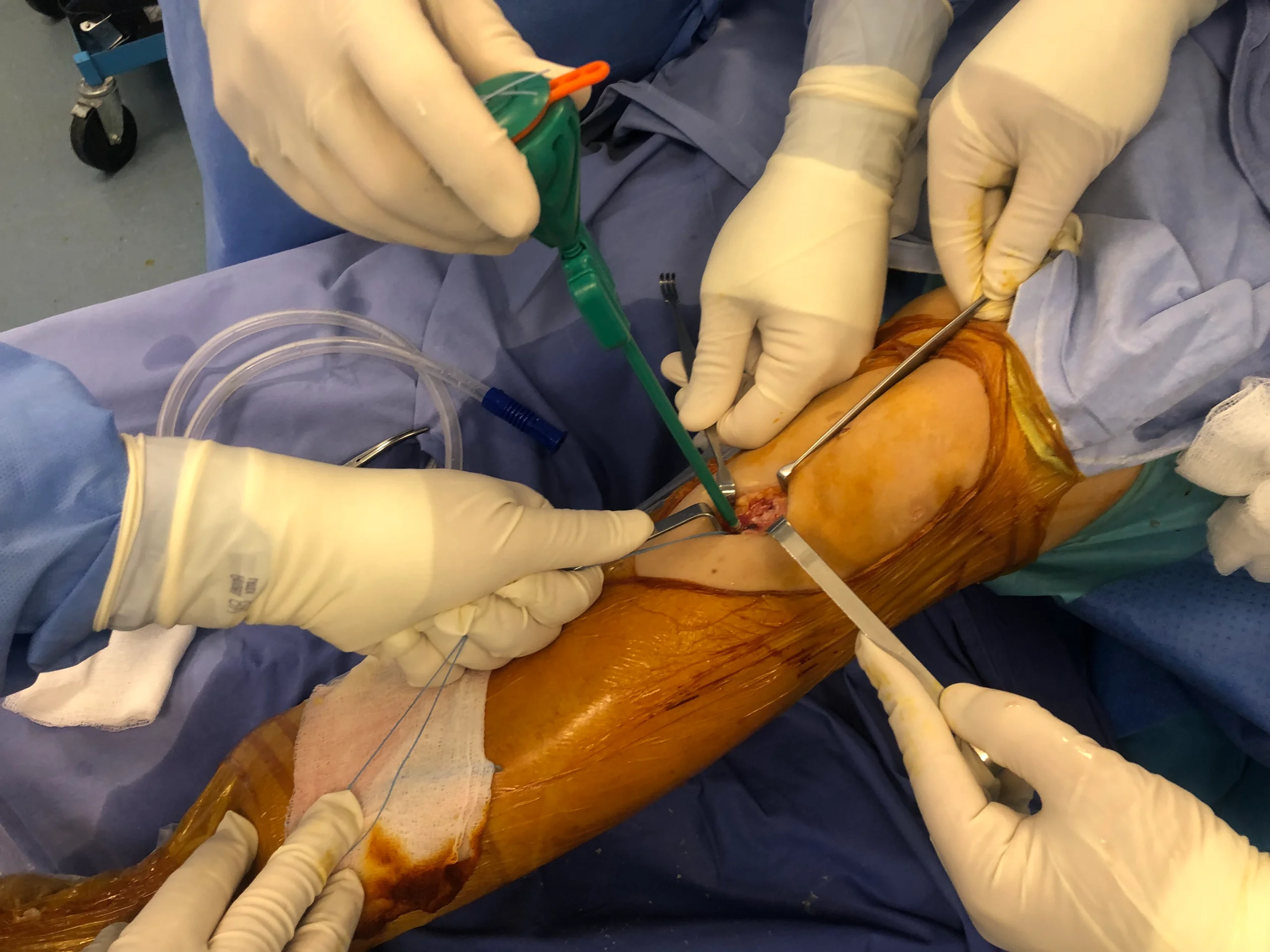
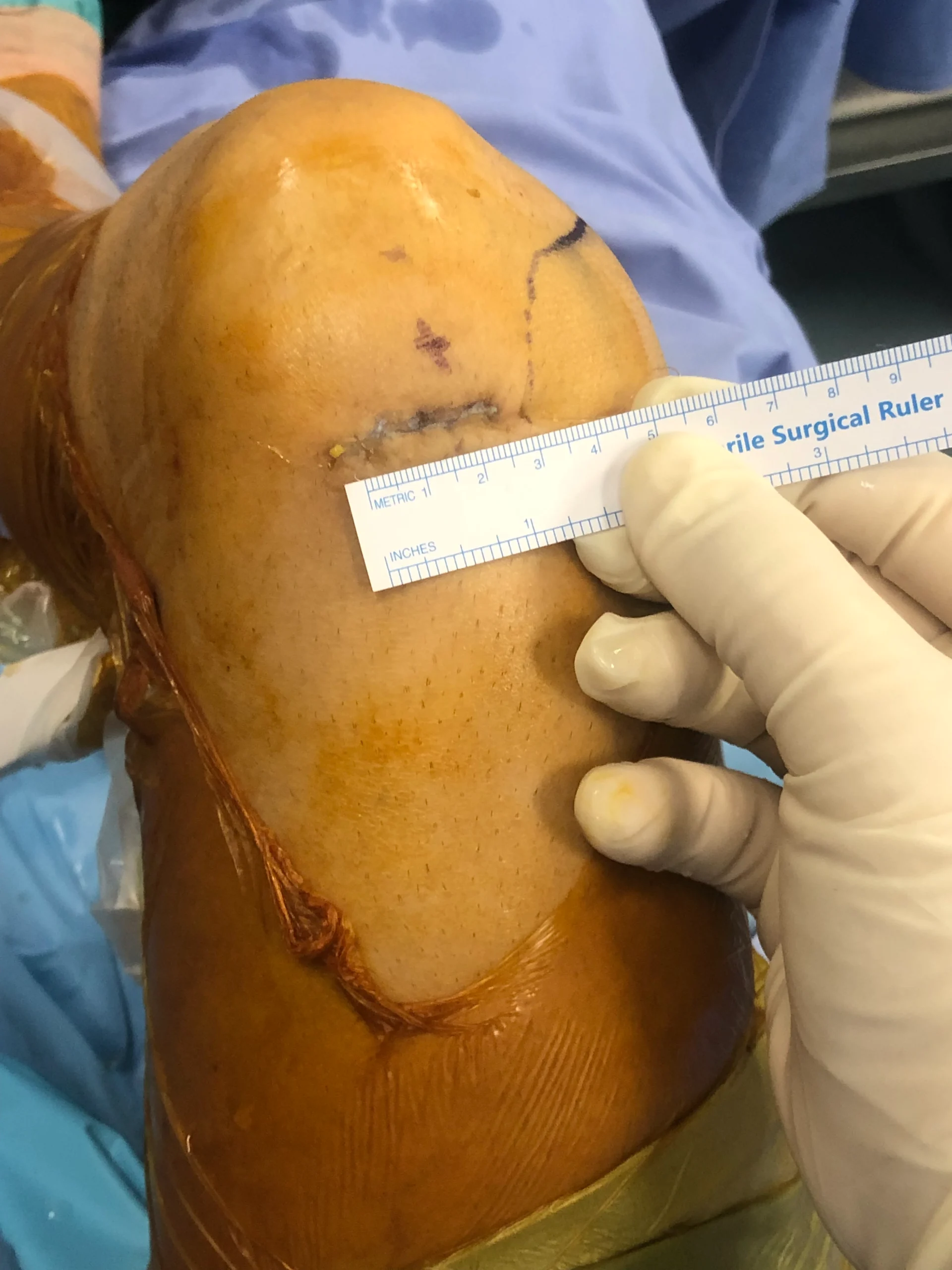
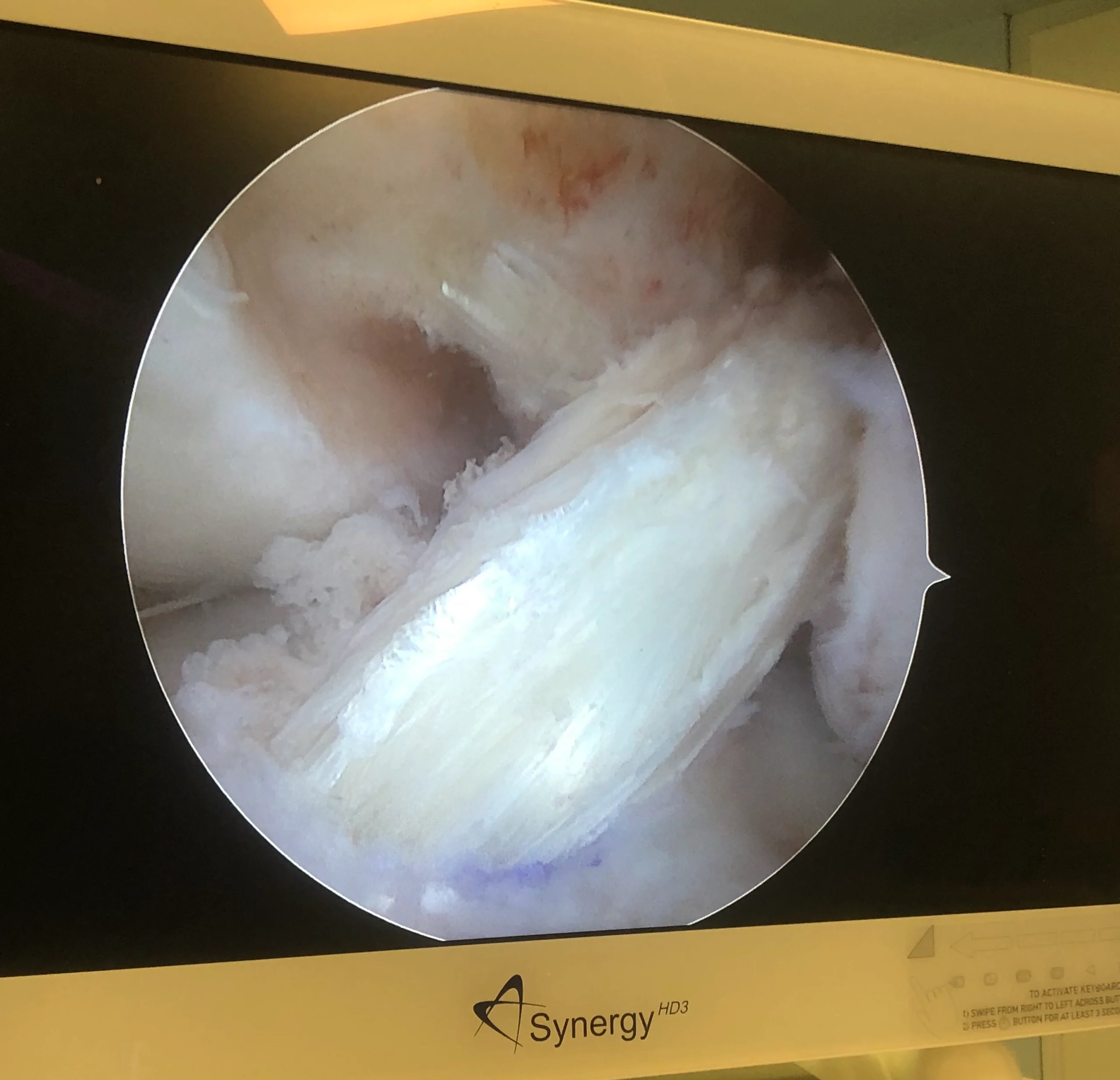
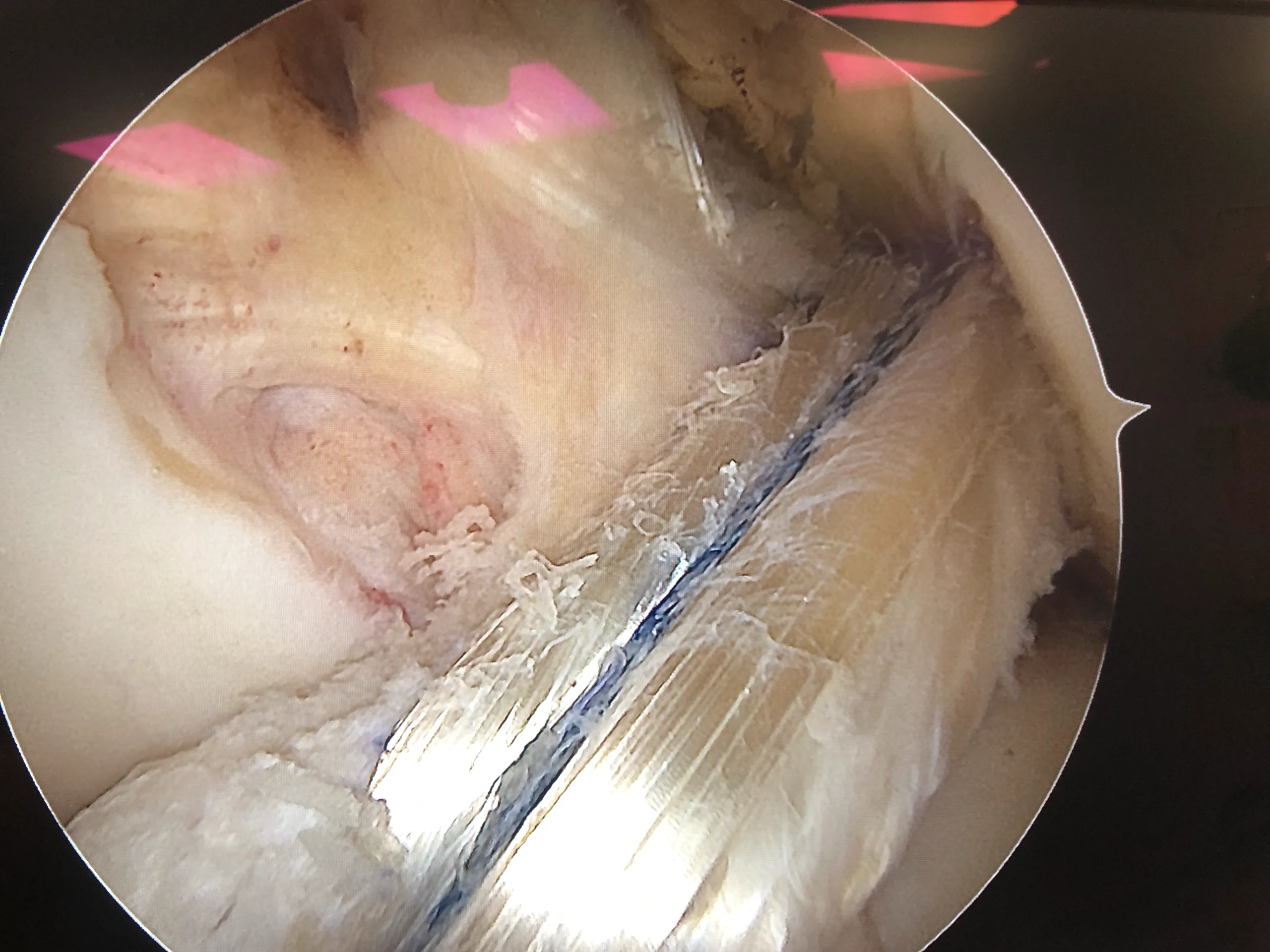
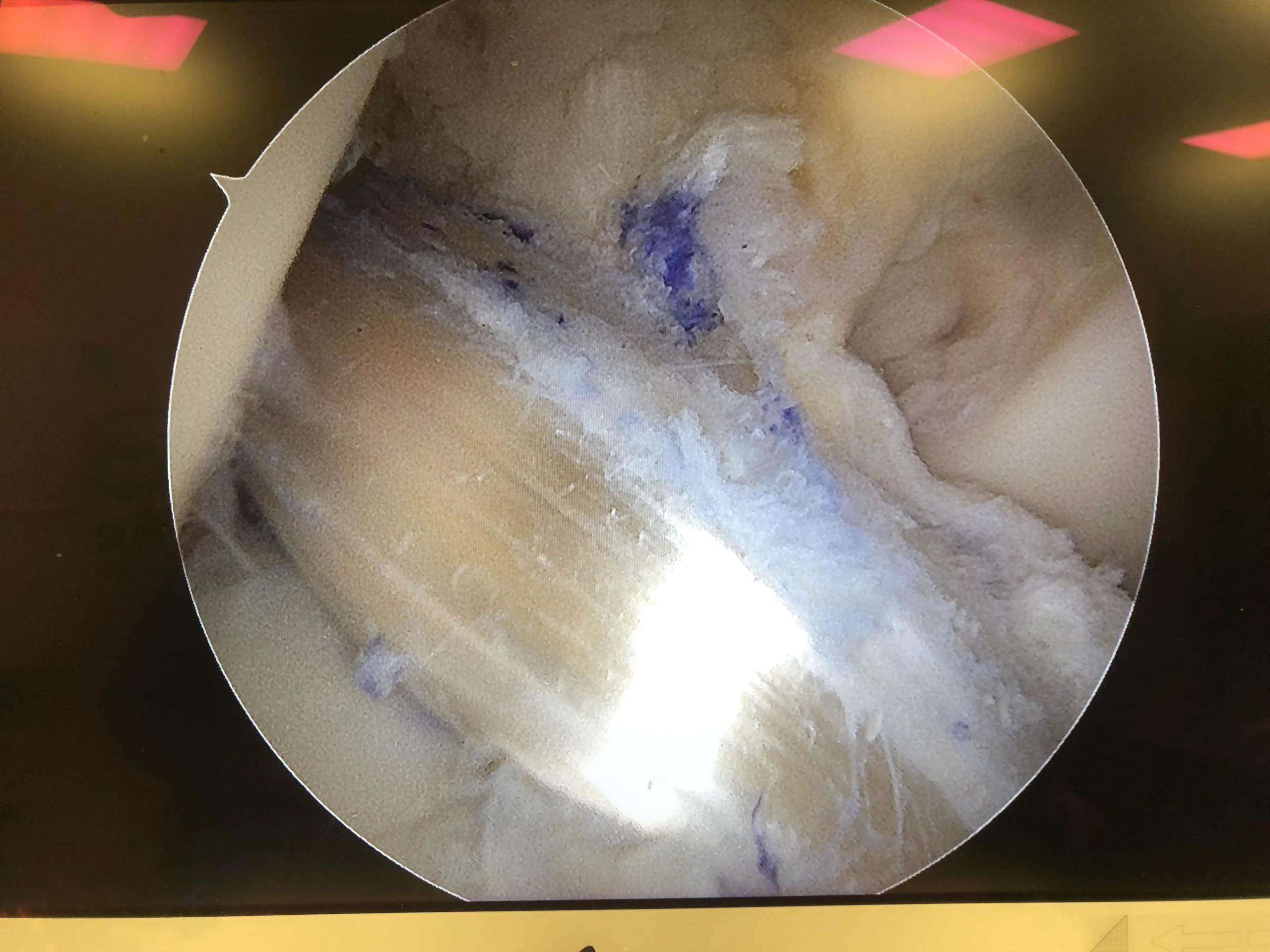
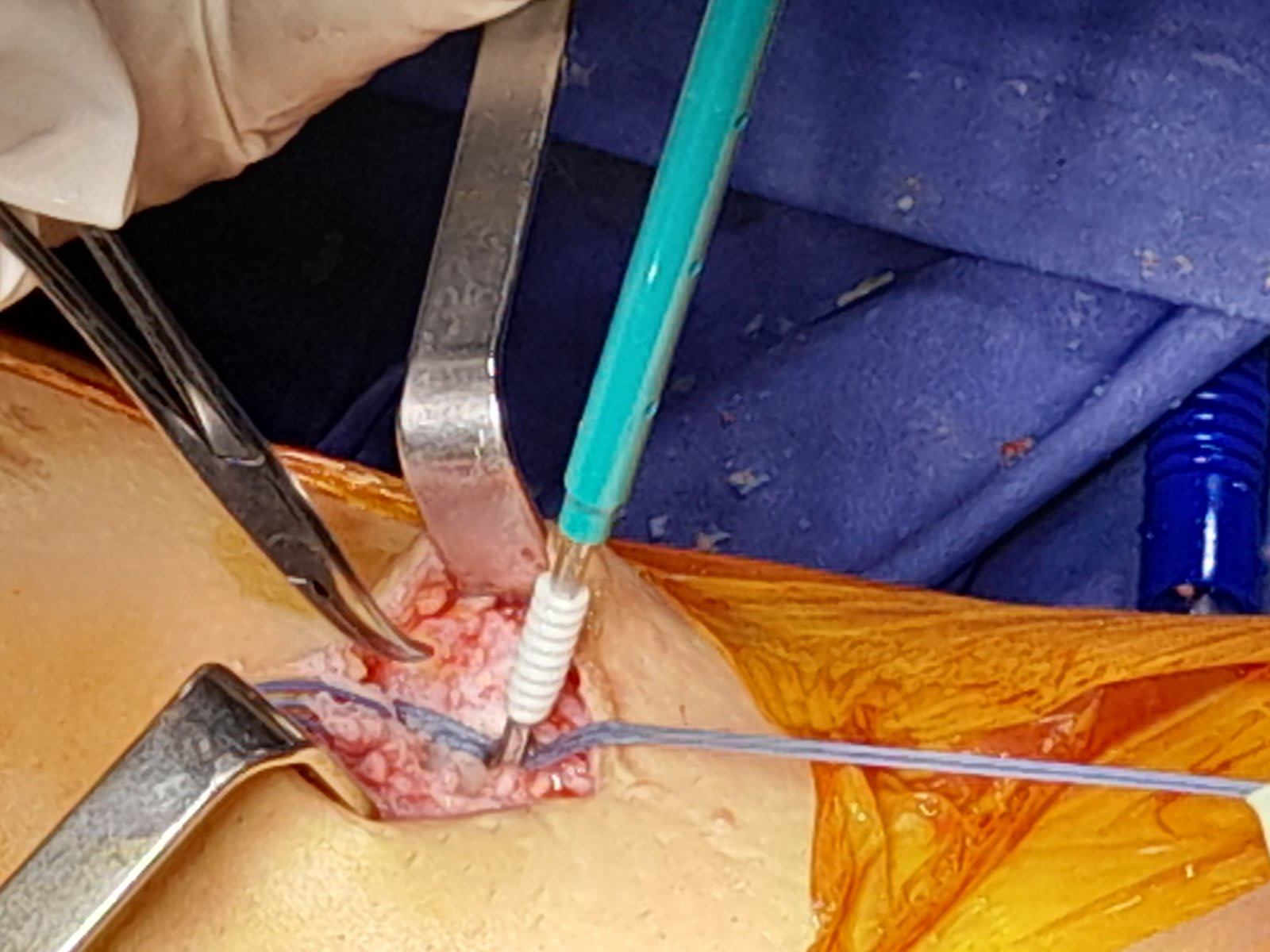
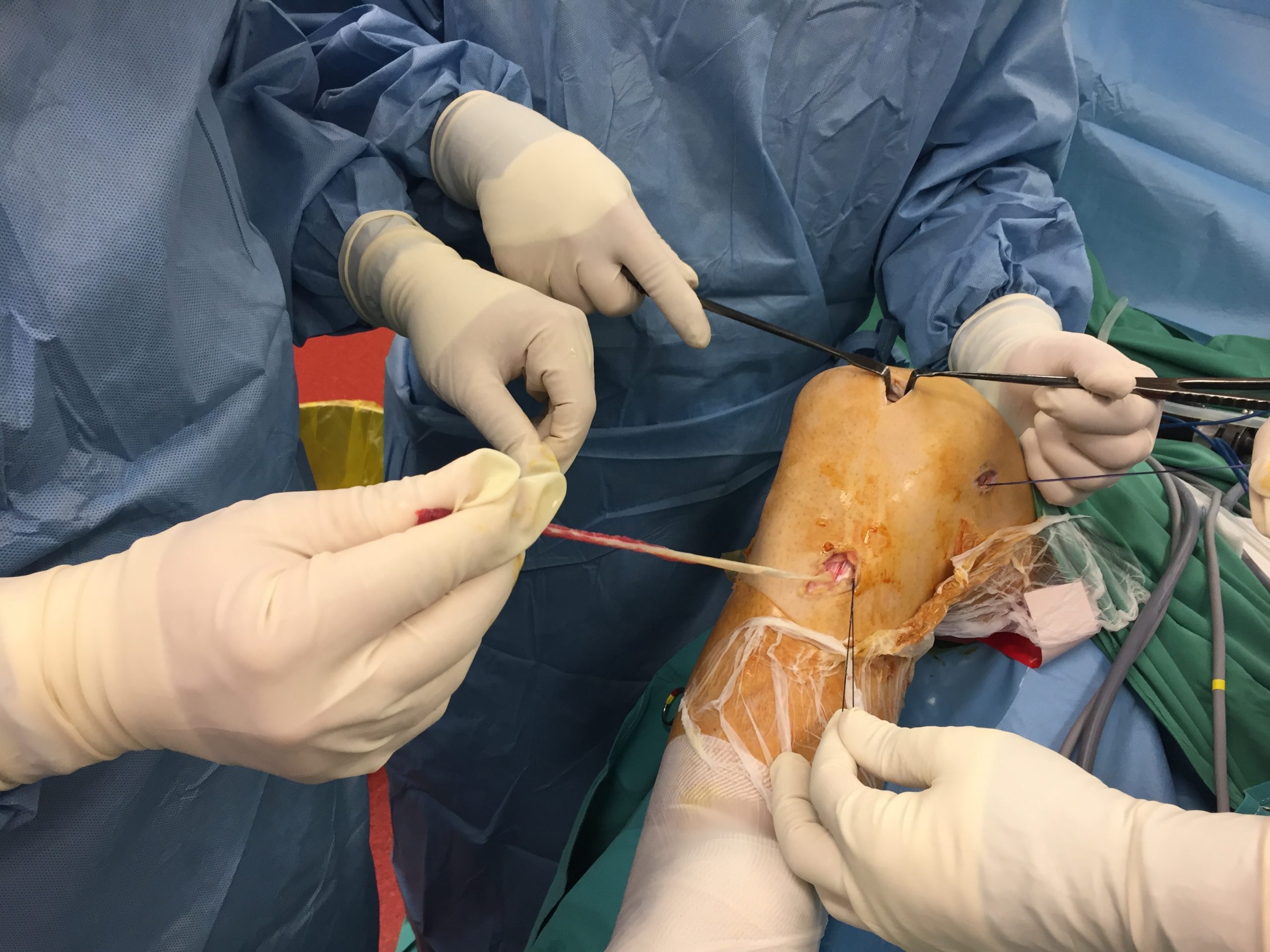
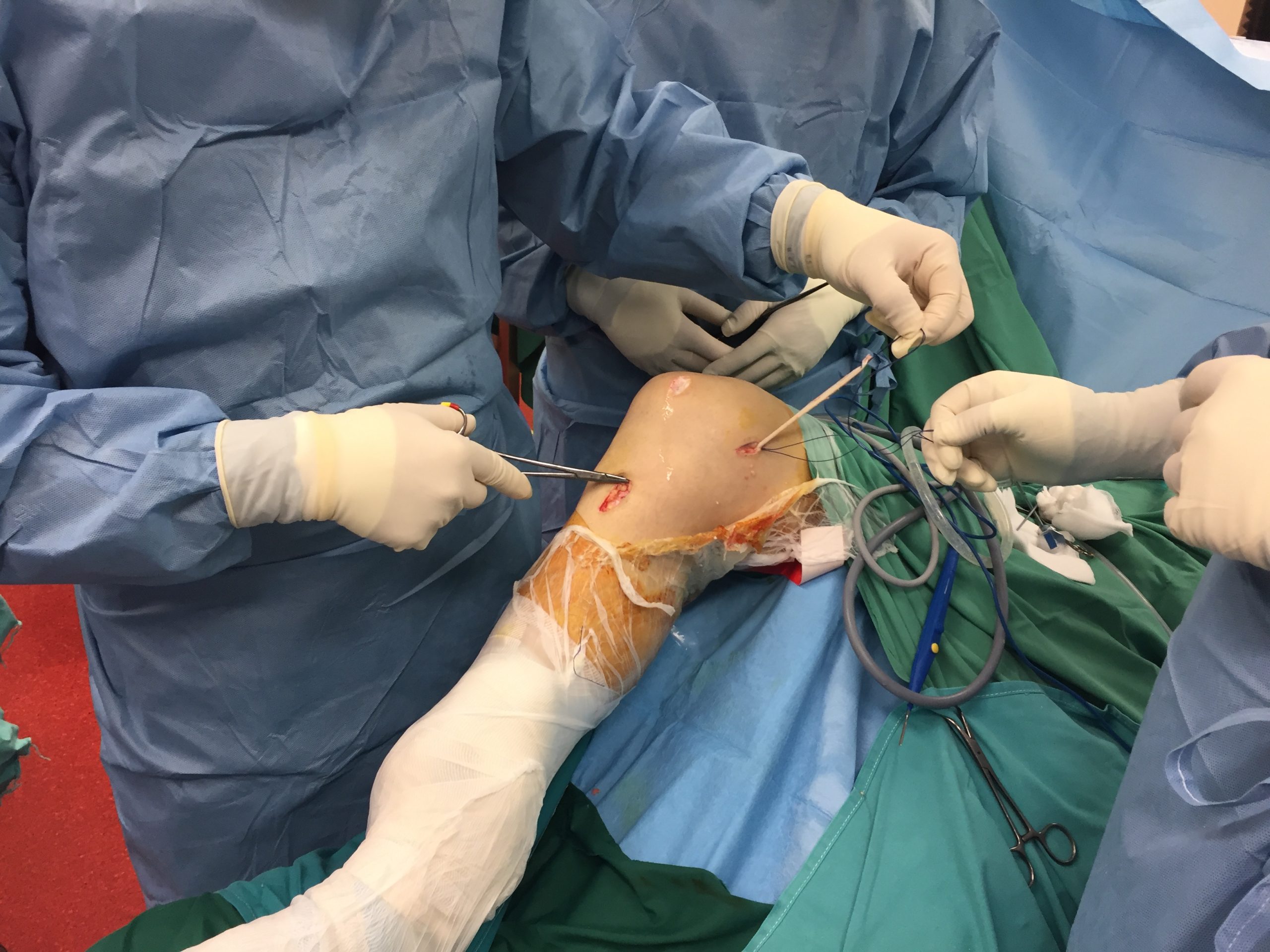
He has performed all kinds of established methods for ACL reconstruction and repair, all grafts, and almost all the best implants. He is currently using hamstrings tendons or only the semitendinosus tendon with Arthrex all inside technique.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- He is using Internal Brace of Arthrex for reinforcement especially in top level athletes, children, women and revisions.
{kind=link}
{kind=link}
He is using the Modified Lemaire Technique Lateral Extra Articular Tenodesis as an adjunct to ACL reconstruction in cases of high risk of graft tear like revision cases or gross rotational instability and the ALL Internal Brace technique.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cartilage Pathology
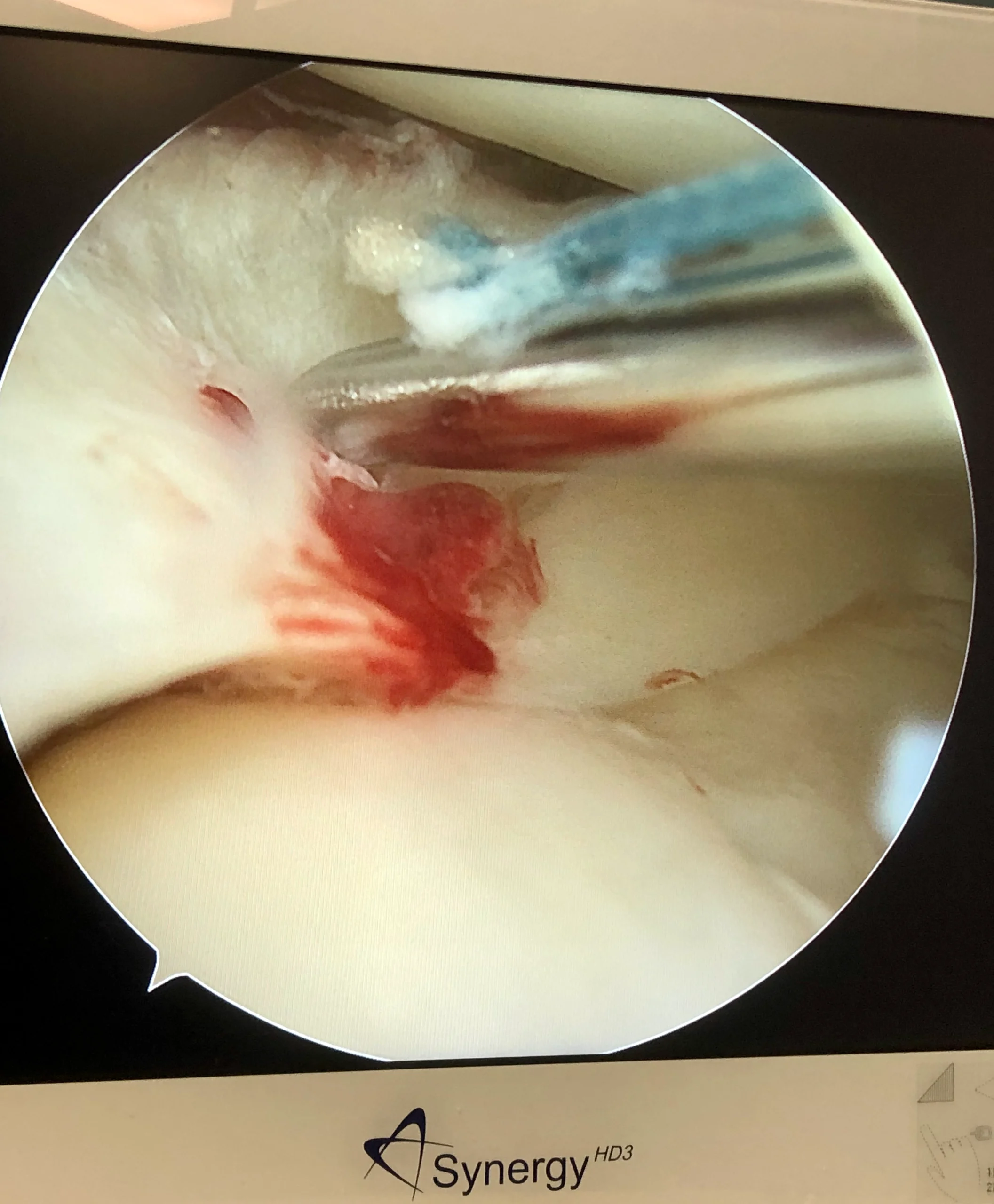
Articular cartilage is the smooth, white tissue that covers the ends of bones where they come together to form joints. Healthy cartilage in our joints makes it easier to move. It allows the bones to glide over each other with very little friction. Articular cartilage can be damaged by injury or normal wear and tear.
Classification of articular lesions by severity
Grade | Outerbridge | Modified Outerbridge | ICRS |
0 | Normal cartilage | Intact cartilage | Intact cartilage |
I | Softening and swelling | Chondral softening or blistering with intact surface | Superficial (soft indentation or superficial fissures and cracks) |
II | Fragmentation and fissures in area less than 0.5 inch in diameter | Superficial ulceration, fibrillation, or fissuring less than 50% of depth of cartilage | Lesion less than half the thickness of articular cartilage |
III | Fragmentation and fissures in area larger than 0.5 inch in diameter | Deep ulceration, fibrillation, fissuring or chondral flap more than 50% of cartilage without exposed bone | Lesion more than half the thickness of articular cartilage |
IV | Exposed subchondral bone | Full-thickness wear with exposed subchondral bone | Lesion extending to subchondral bone |
From ICRS: International Cartilage Repair Society
Our good friend and mentor Prof. Mats Brittberg was the first to report Autologous chondrocyte implantation (ACI) in 1994. Being a two-stage technique, the first stage in ACI involves an arthroscopic evaluation of the chondral lesion and biopsy by harvesting of chondrocytes. We are now at the 3-4th generation of cartilage restoration with a one-stage procedure using minced cartilage, autologous stem cells from bone marrow and chondrocytes. Excellent is the Autocart Arthrex technique.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bone Marrow Edema ( bone Bruise- lesion)
A bone bruise is thought to occur when there is a microscopic fracturing of the internal bone structure. While these microfractures don’t significantly weaken the bone, they can cause bleeding and inflammation within the bone. This can lead to pain and symptoms similar to a more familiar soft-tissue bruise.
Vascular anomalies, decreased fibrinolysis (especially in pregnant women), and thromboembolism have all been proposed as possible etiologies, but a definitive cause remains elusive. Ultimately, the pain is likely caused by the aggravation of neurovascular bundles within the bone marrow due to increased intraosseous pressure caused by the increased fluids in the bone marrow interstices.
It can be caused by injury, arthritis, osteoporosis, tumors, or infections. It is frequently misdiagnosed as its clinical presentation is highly variable and nonspecific. As such, it may be referred to by many terms, including “transient osteoporosis,” “regional migratory osteoporosis,” and “algodystrophy.”
The diagnosis is based on the MRI, with high bone marrow signal T2, fluid sensitive, fat depressed.
The three O’s are the goal of the treatment: promote healing: osteoconduction–osteoinduction–osteogenesis.
Non-weight bearing (activity modification), anti-osteoporotic drugs, vitamins (bisphosphonates and vitamin D supplementation), special physiotherapy machines, and hyperbaric oxygen treatments constitute the conservative treatment.
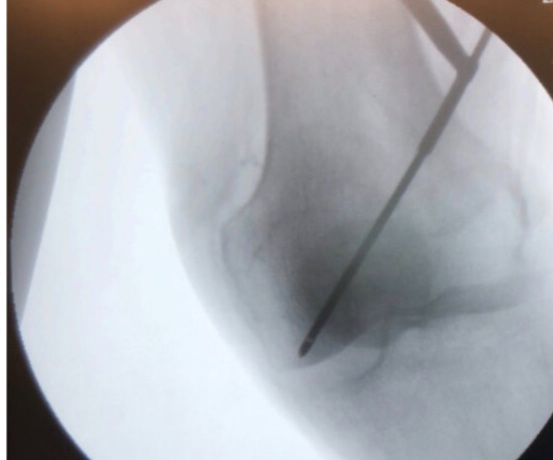
In cases of persistent bone bruise, osteoarthritis, and early stages of avascular necrosis, we are doing a core decompression of the lesion and direct application of PRP and bone marrow concentrate stem cells according to the Intraosseous Bioplasty IOBP/Biofiller technique of Arthrex. We also use microfragmented-fat delivered intraosseous and intraarticular under arthroscopic and fluoroscopic control.
{kind=link}
{kind=link}
{kind=link}
Patellar Dislocation-instability
Patellar instability is a condition characterized by patellar subluxation or dislocation episodes as a result of injury, ligamentous laxity, or increased Q angle of the knee. Diagnosis is made clinically in the acute setting with a patellar dislocation with a traumatic knee effusion and in chronic settings with passive patellar translation and a positive J sign. MRI and CT-scan are very useful. Treatment is nonoperative with bracing for first-time dislocation without bony avulsion or presence of articular loose bodies. Operative management is indicated for chronic and recurrent patellar instability. Arthroscopic debridement (removal of loose body) vs Repair with or without stabilization. Indications: displaced osteochondral fractures or loose bodies may be an indication for operative treatment in a first-time dislocator. MPFL reconstruction with autograft vs allograft. Indications: recurrent instability/ no significant underlying malalignment. Techniques: gracilis or semitendinosus commonly used (stronger than native MPFL)/ femoral origin can be reliably found radiographically (Schottle point)/a femoral tunnel positioned too proximally results in graft that is too tight (“high and tight”)/in pediatric patients, femoral side should be secured more anterior/distal to Schottle’s point. Severe trochlear dysplasia is the most important predictor of residual patellofemoral instability after isolated MPFL reconstruction. Trochleoplasty is an arthroscopic or open trochlear deepening procedure in severe cases.Different kinds of osteotomies, like Fulkerson-type osteotomy, anterior and medial tibial tubercle transfer, may be needed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Osteochondritis Dissecans
- Osteochondritis Dissecans is a pathologic lesion affecting articular cartilage and subchondral bone.
- Diagnosis may be made radiographically (notch view) but MRI usually required to determine size and stability of lesion, and to document the degree of cartilage injury.
- Treatment may be nonoperative with restricted weight bearing in children with open physis. Surgical treatment may be indicated in older patients (closed physis), lesions that are unstable and patients who have failed conservative management.
| ||
|
| |
|
| |
|
| |
|
|
|
Operational treatment according to the stage:
Subchondral drilling with K-wire or drill/ fixation of unstable lesion /chondral resurfacing.