Arthritis-Osteoarthritis
Based on the severity of the osteoarthritis and the Kellgren-Lawrence classification
- grade 0 (none): definite absence of x-ray changes of osteoarthritis
- grade 1 (doubtful): doubtful joint space narrowing and possible osteophytic lipping
- grade 2 (minimal): definite osteophytes and possible joint space narrowing
- grade 3 (moderate): moderate multiple osteophytes, definite narrowing of joint space, some sclerosis and possible deformity of bone ends
grade 4 (severe): large osteophytes, marked narrowing of joint space, severe sclerosis and definite deformity of bone ends
we apply the following protocol!
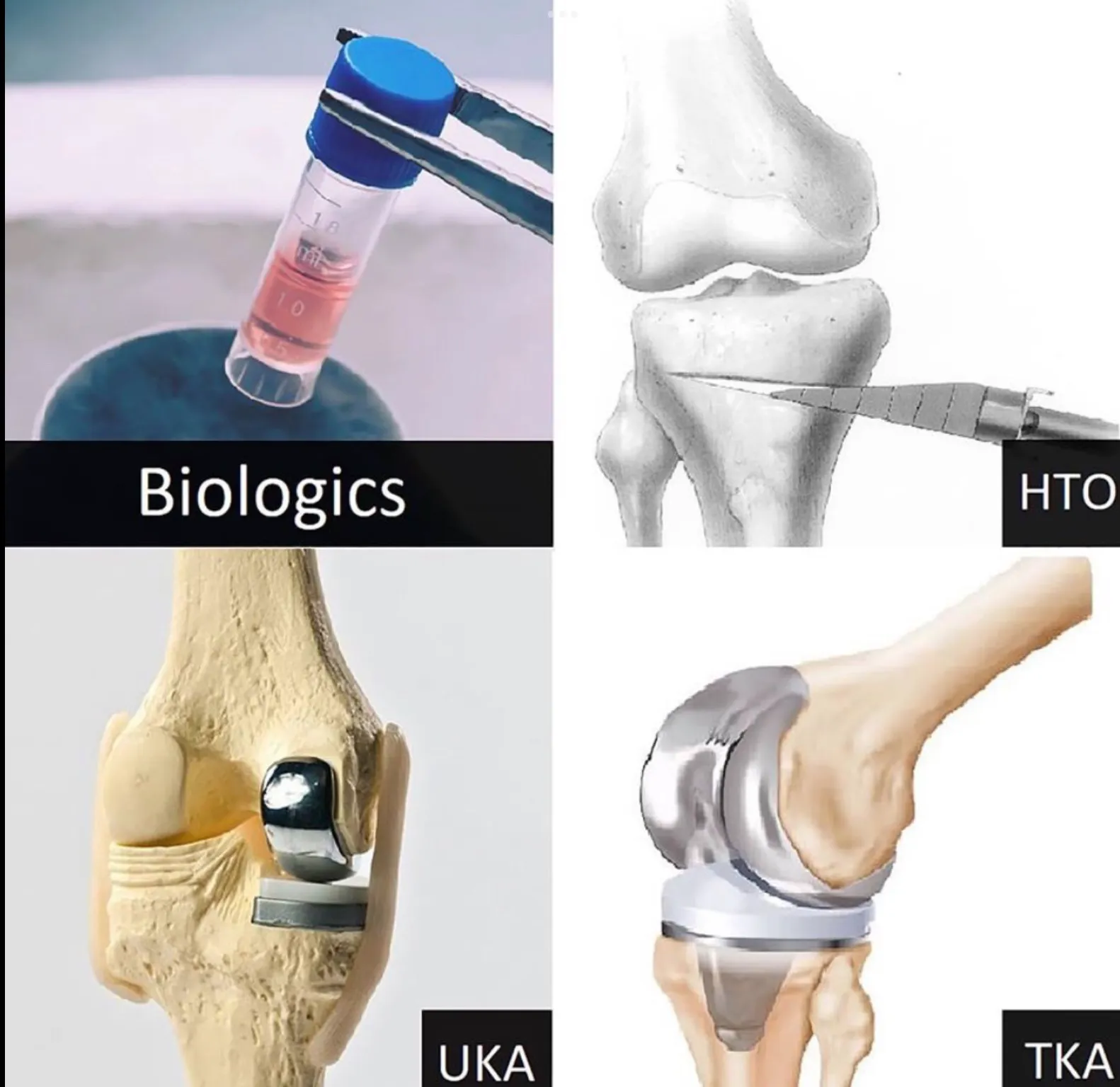
- Injections_Orthobiologics
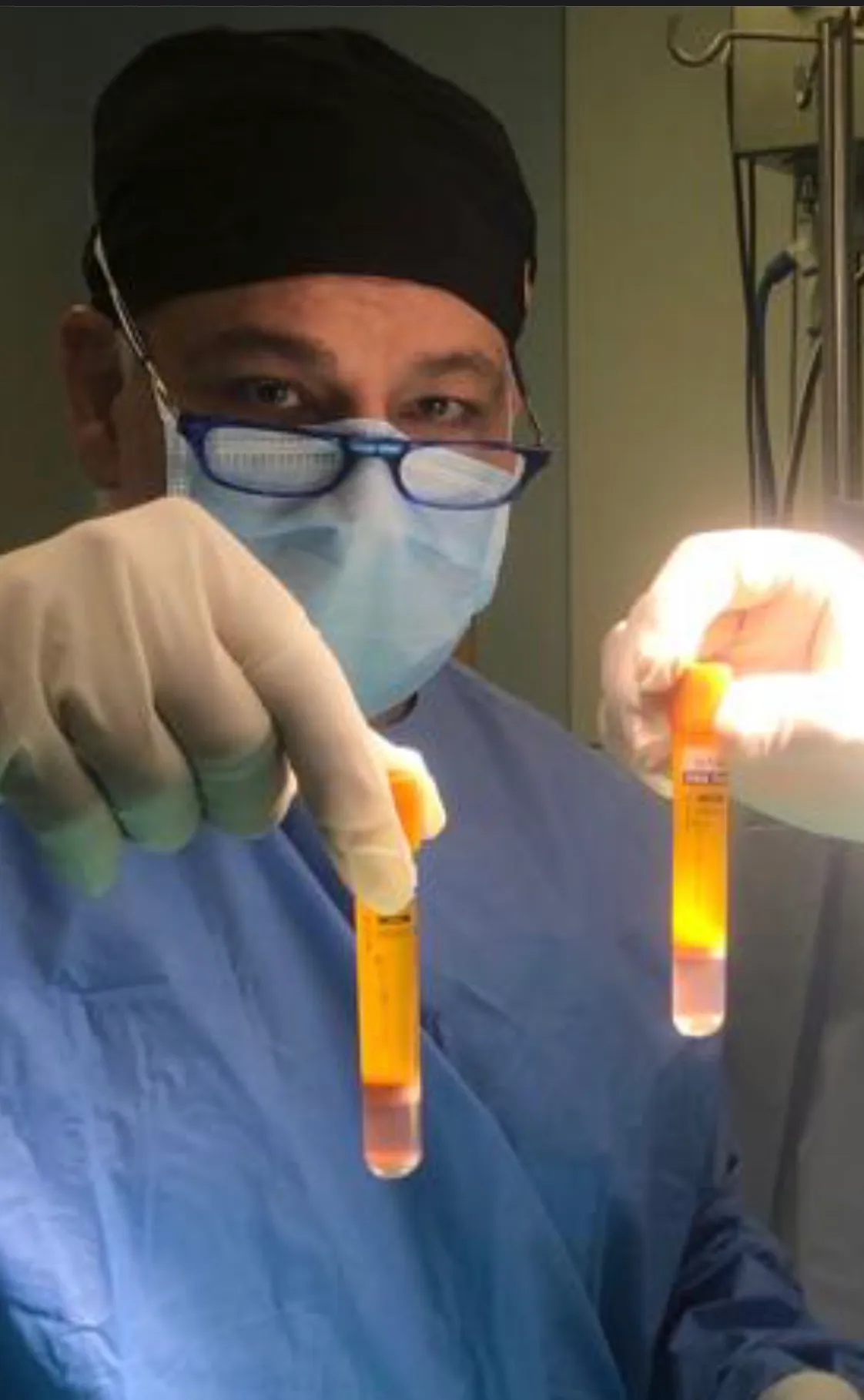
For arthritis K-L stage 2 early 3 we use intra-articular and sometimes intra-osseous PRP, platelet rich plasma, injections with or without Photobiomodulation under ultrasound guidance. Be careful! All PRP are not created equal and different kinds of PRP , like LR-PRP/ LP-PRP/PPP, have different indications.
The three best indications for PRP are elbow tendinopathy/ gluteal tendinopathy/ knee osteoarthritis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
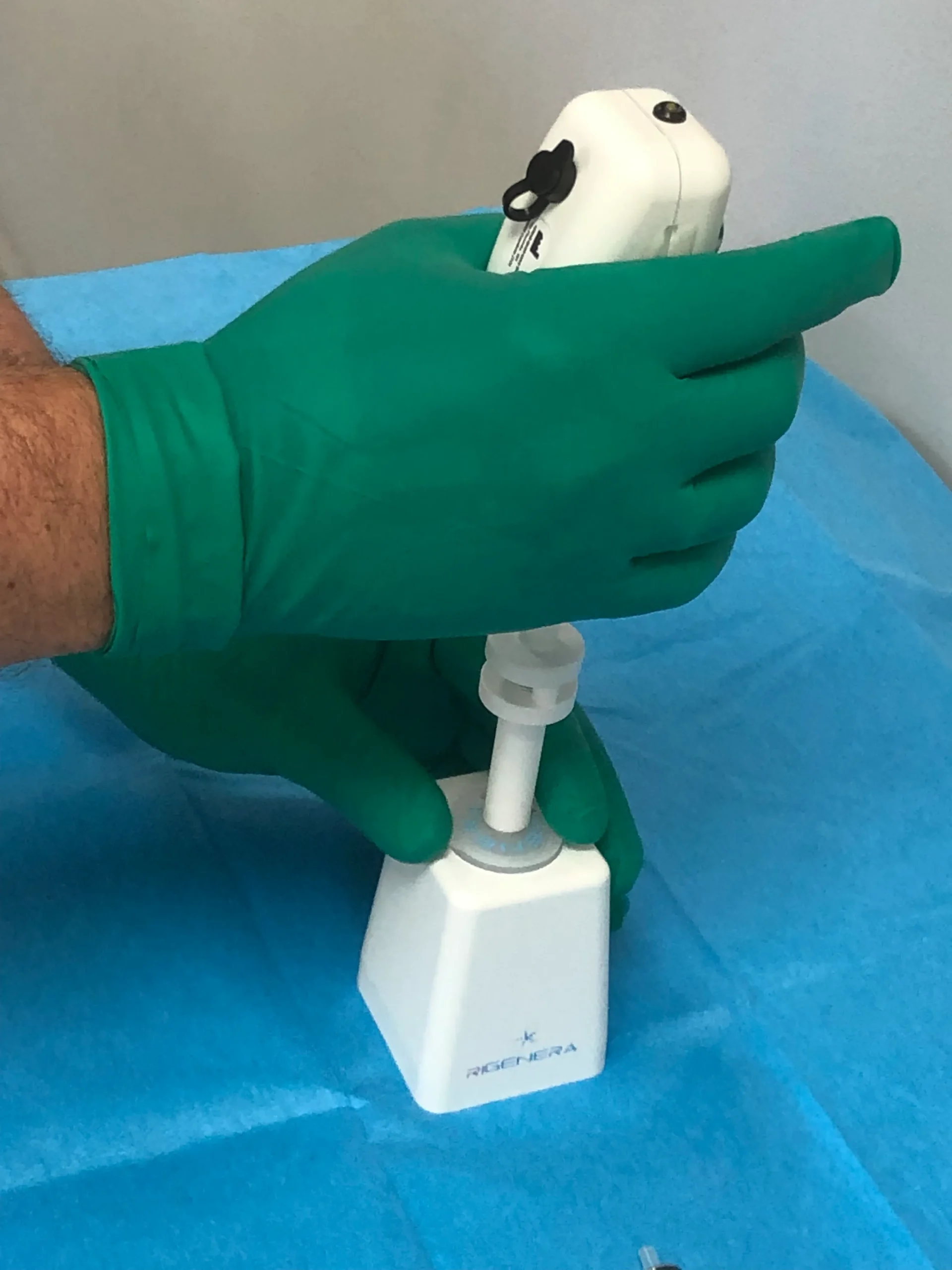
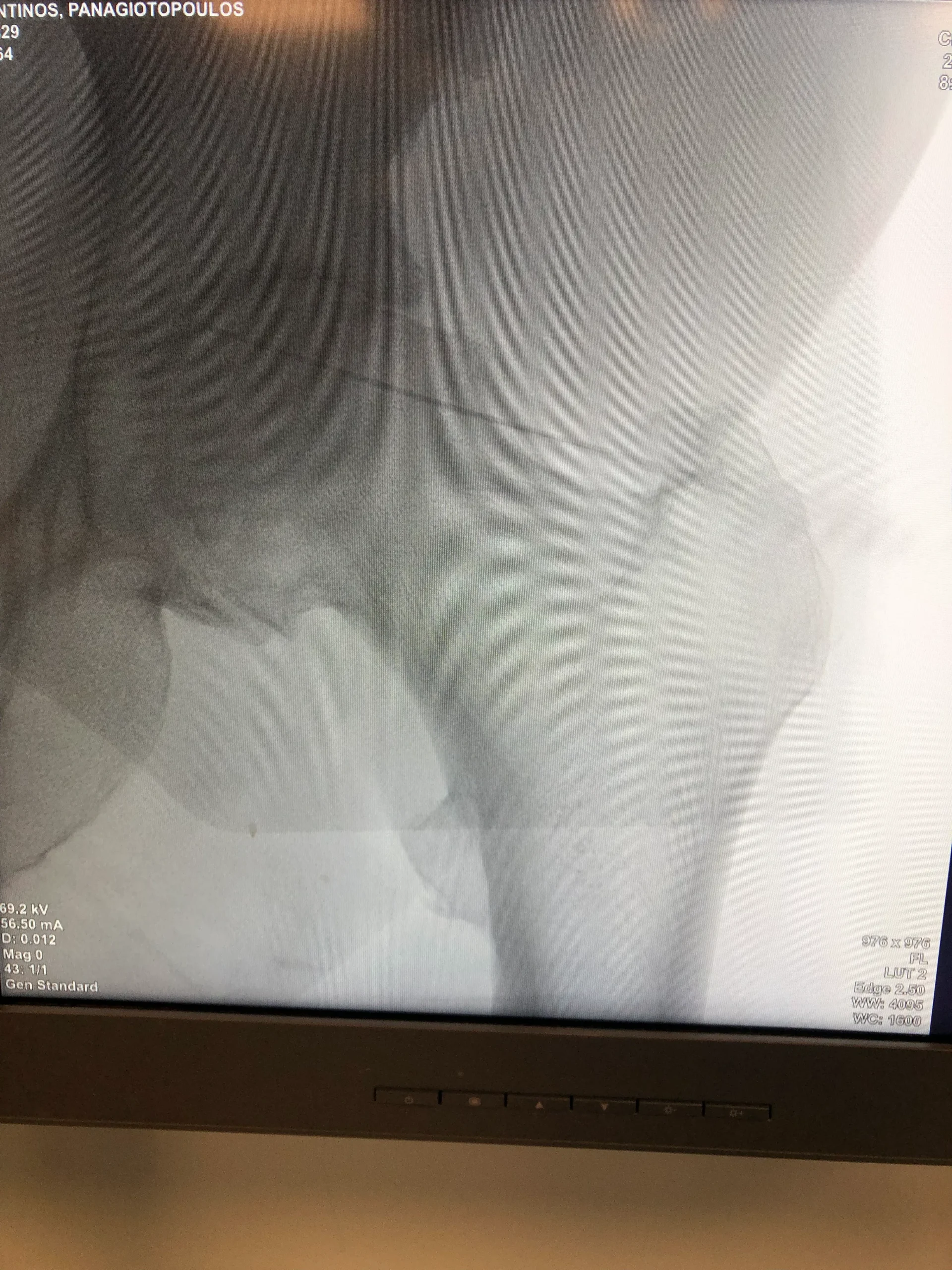
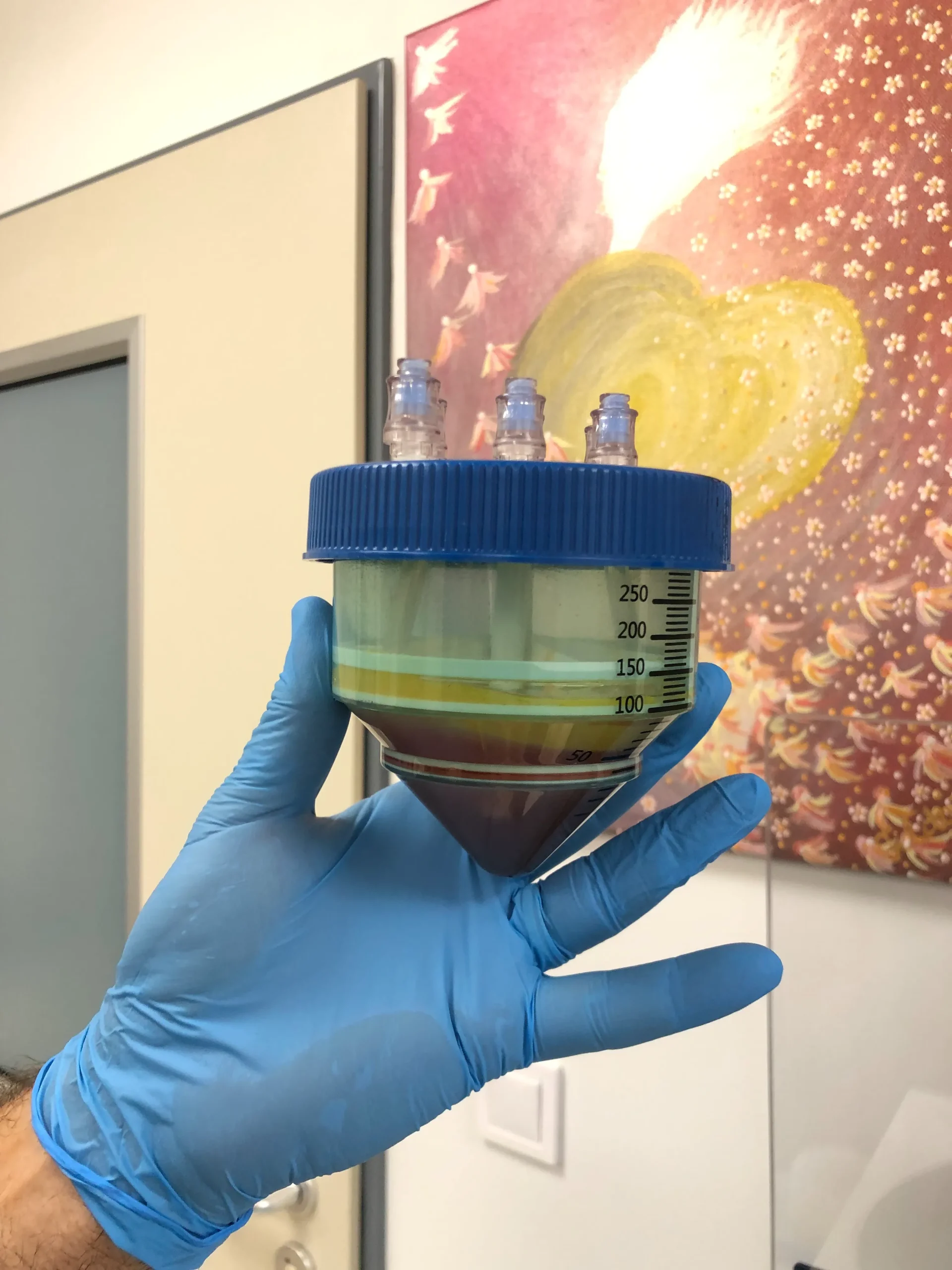
For arthritis stage K-L 3 early 4 and sometimes 4 we use stem cells intraarticular injections with or without arthroscopy. We have more than 12 years of experience in this kind of treatment. In younger ages we prefer mesenchymal stem cells from Bone Marrow concentrate according the Arthrex technique, from the iliac spine.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In order to obtain the fat fom the belly Dr. Tsoukas, trained and certified by Prof. Plastic Surgeon, performs a minor lipoaspiration, the first Orthopaedic Surgeon who did that in Greece and Cyprus and trained other doctors in Spain, Norway, Israel, Azerbaijan and Hungary.
Dr. Tsoukas is an accredited global instructor of these techniques .
He was also the first Orthopaedic Surgeon in Europe who performed a Knee lipoaspiration ! for the Lipopras technique of adipose derived stem cells.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The first technique he applied almost 12years ago was that of Harvest-Terumo.
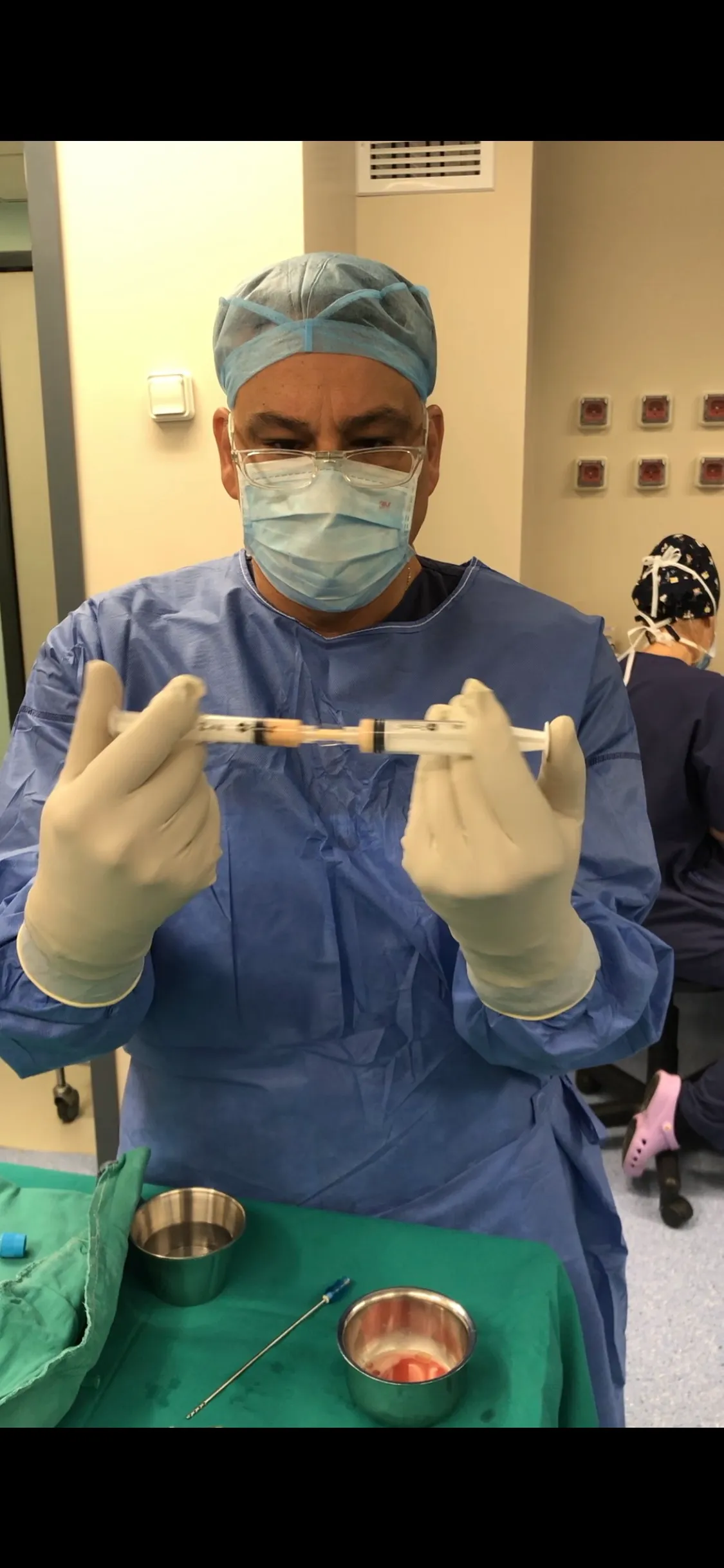
Each one of the above procedures need light sedation in the operation theatre and last about 1 hour. When the patient is ready he can go back home with complete instructions about activity, supplementation, diet, physiotherapy and exercise. The results, if the indications are right, are excellent for 3-4 years with less pain, better mobility easier daily and light sport activities according to ours and hundreds other published studies.
These techniques are the best choice for a patient who is not ready for metals and knee or hip arthroplasty yet or for a patient who has many health issues that don’t allow him to undergo a difficult operation.
Knee Osteotomy
High tibia osteotomy (HTO) is intended to transfer the mechanical axis from medial to slightly lateral to the midline of the knee to decrease the load and subsequently delay osteoarthritis (OA) . An ideal patient for HTO is a moderately active high-demand (but not jumping or running), young (between 40-60 years old) with isolated medial joint line tenderness, BMI <30, malalignment <15°, metaphyseal varus, full range of motion (ROM), near-normal lateral and patellofemoral compartments, without ligamentous instability, non-smoker.
We perform the new biplanar HTO.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Unicompartmental knee arthroplasty (UKA) is a procedure for the treatment of unicompartment femoro-tibial arthritis. Current indications for UKA implantation are: unicondylar osteoarthritis (OA) or osteonecrosis; frontal deformity < 15°; flexion contracture < 15°; functional integrity of the anterior cruciate ligament and peripheral ligaments of the knee as well as the absence of an inflammatory arthropathy. UKA implantation for anteromedial OA requires medial bone-on-bone arthritis, a functionally normal ACL, a functionally normal medial collateral ligament, intact full-thickness lateral cartilage and a patellofemoral joint (PFJ) with no lateral grooving and bone loss.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}