25 ans d'expérience dans le domaine du genou
Le Dr Tsoukas possède plus de 25 ans d'expérience en chirurgie du genou et en arthroscopie. Il est l'un des plus grands spécialistes mondiaux du genou
Rupture du ligament croisé antérieur (LCA). Reprise chirurgicale du LCA
Le Dr Tsoukas a réalisé sa première reconstruction du ligament croisé antérieur en novembre 1999 ! Le patient (AD) était un basketteur qui a joué avec succès pendant 20 ans à haut niveau , en Grèce et à l’étranger, après l’opération . Il est resté très ami avec le Dr Tsoukas.

Un héritage de leadership en chirurgie du LCA
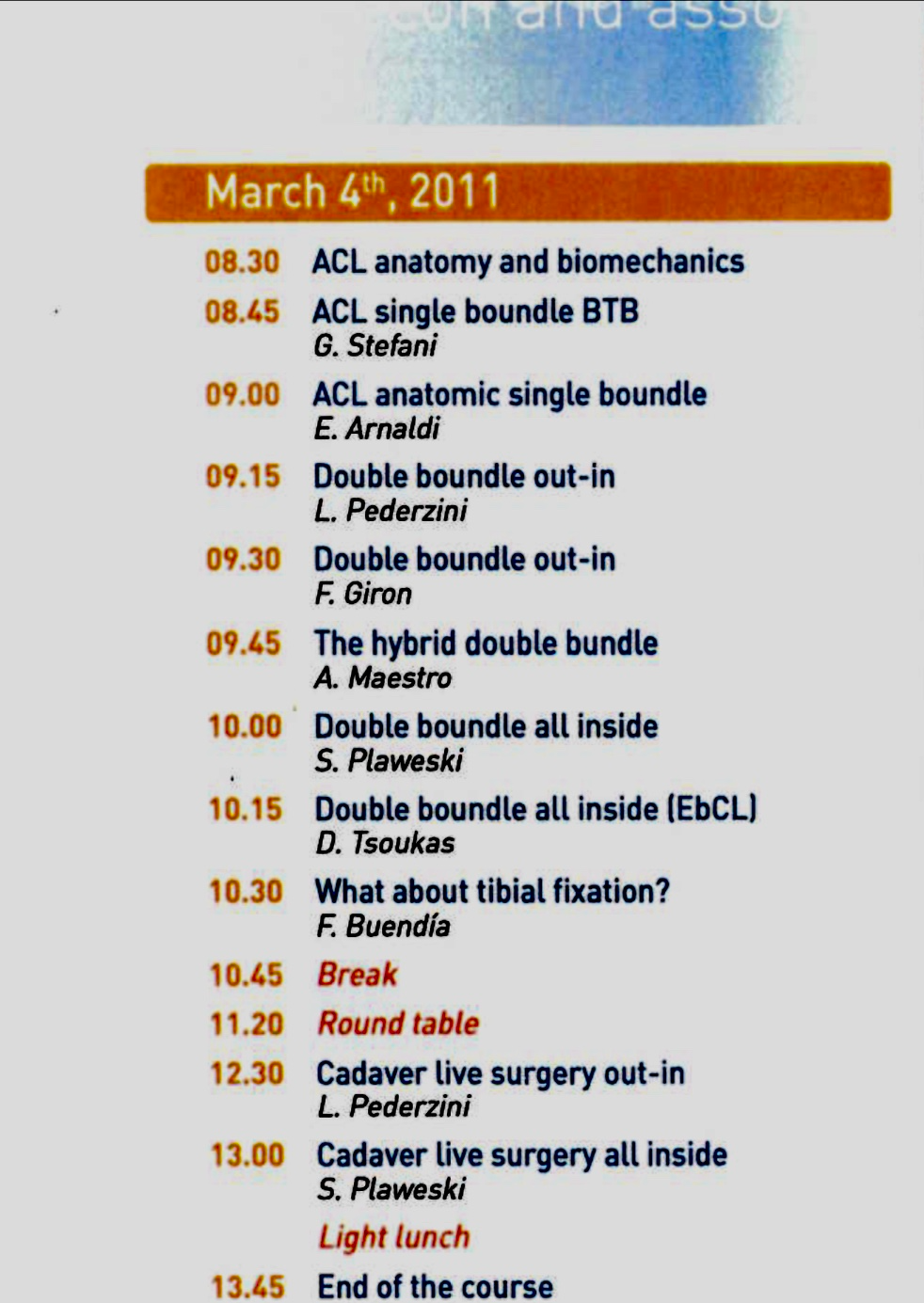
Le Dr Tsoukas était un chirurgien de premier plan chez Smith N Nephew et l'un des tout premiers instructeurs à York, au Royaume-Uni, en 2011 , ainsi que membre du conseil consultatif sur le genou de la société. Il est aujourd'hui l'un des chirurgiens de premier plan d'Arthrex et instructeur à ArthroLab Munich.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rupture du ligament croisé antérieur (LCA). Reprise chirurgicale du LCA
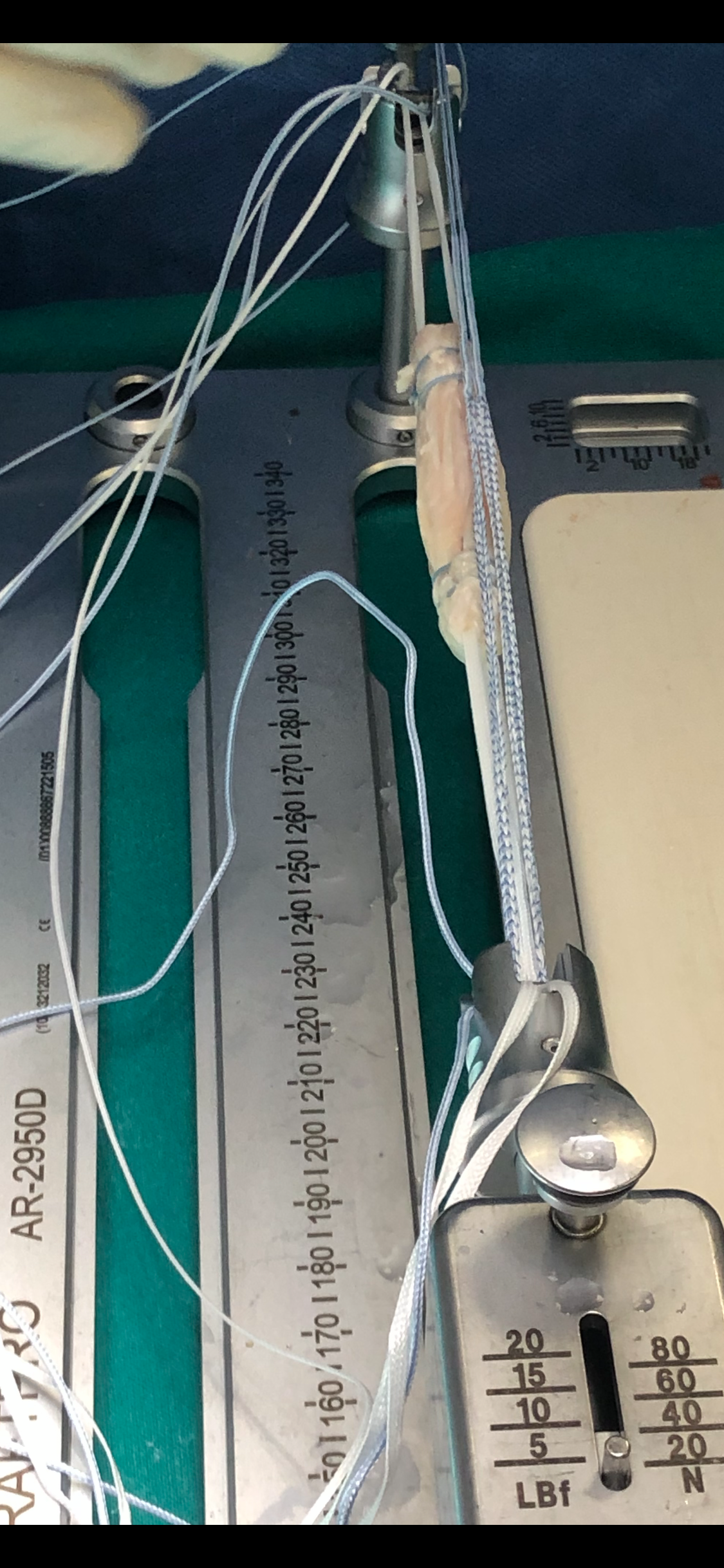
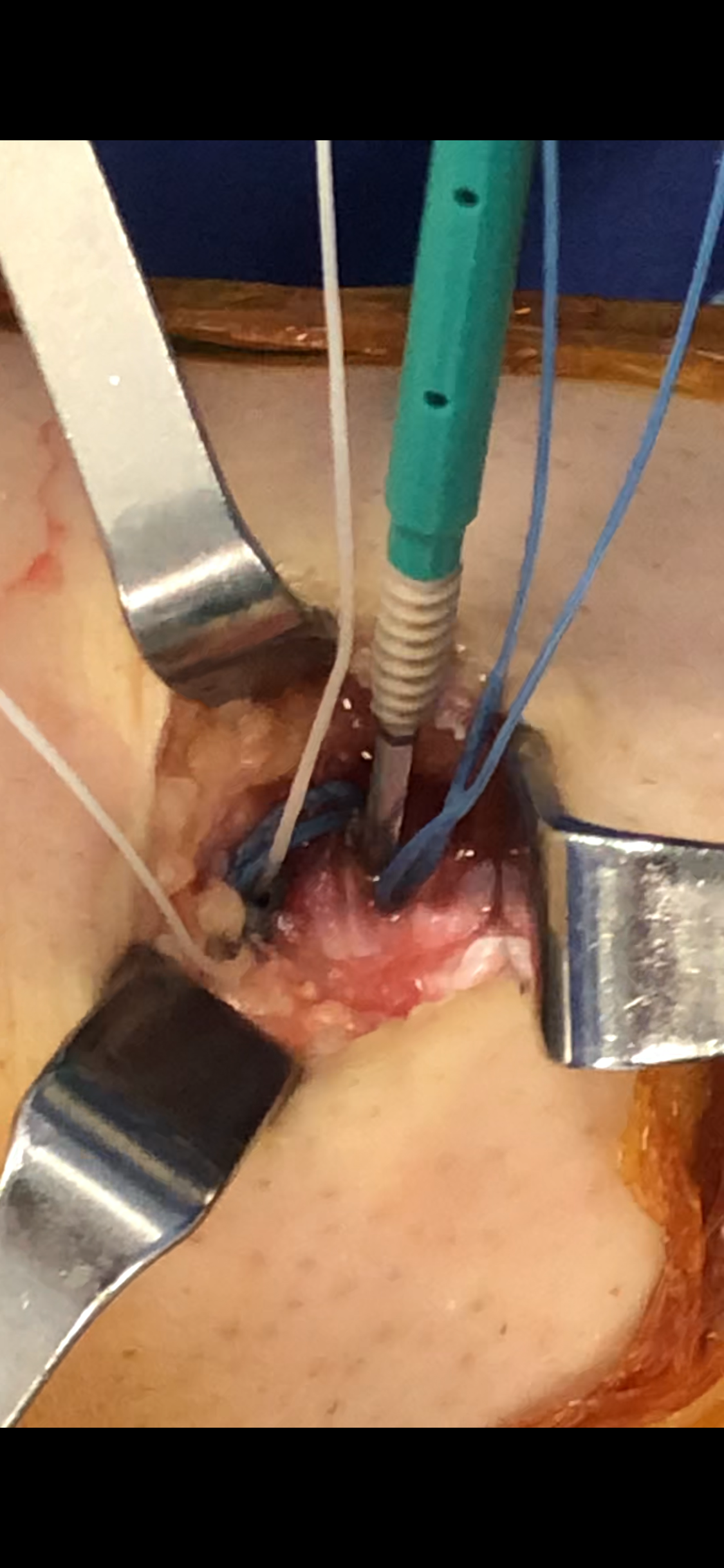
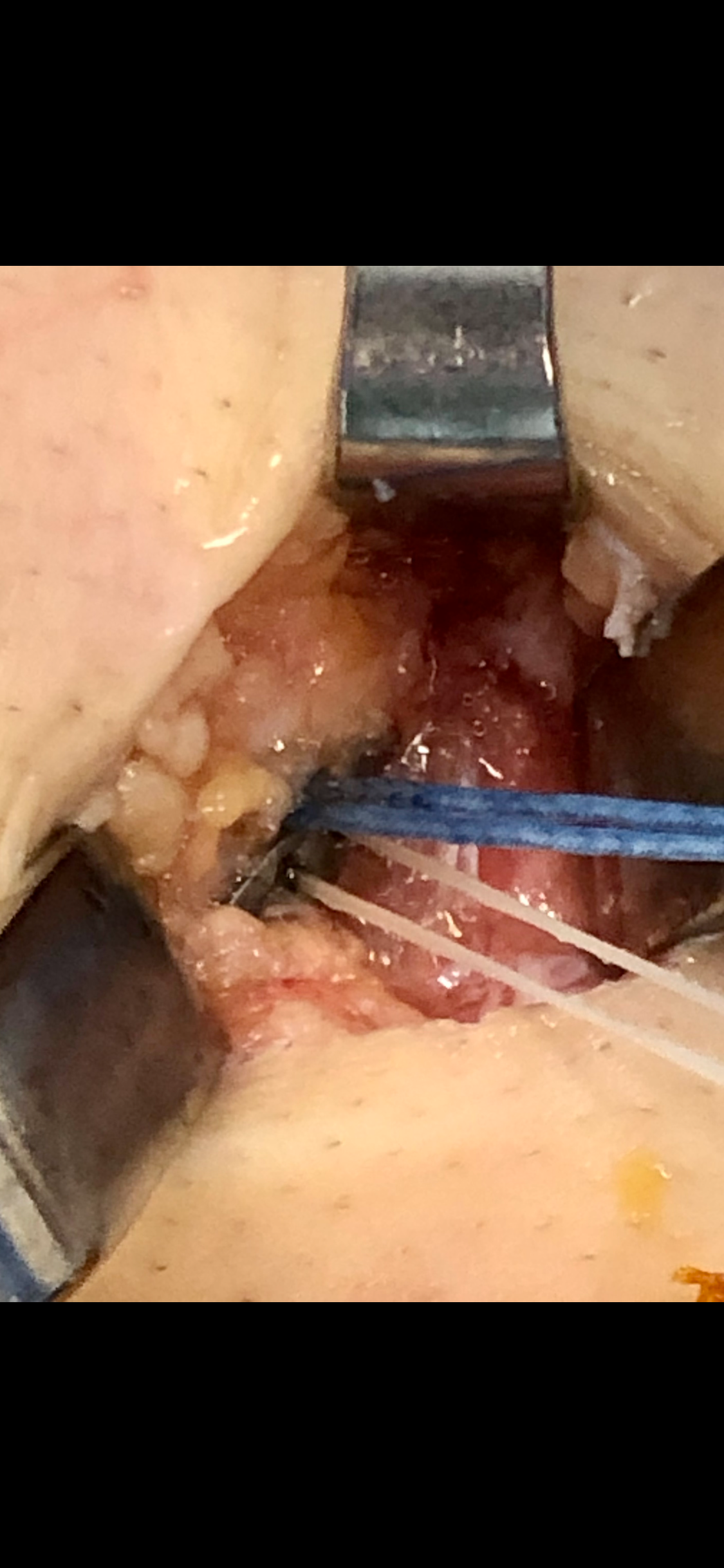
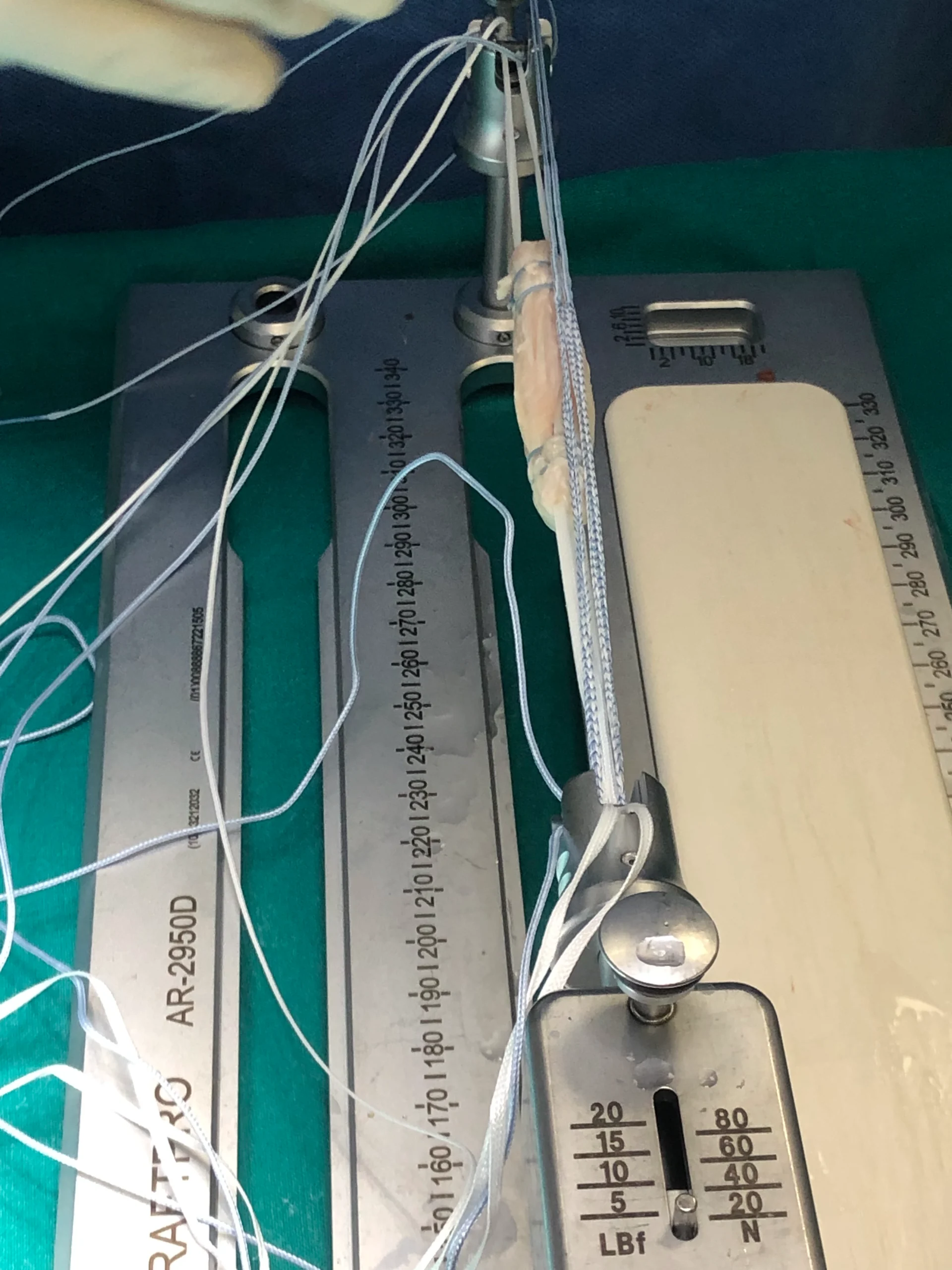
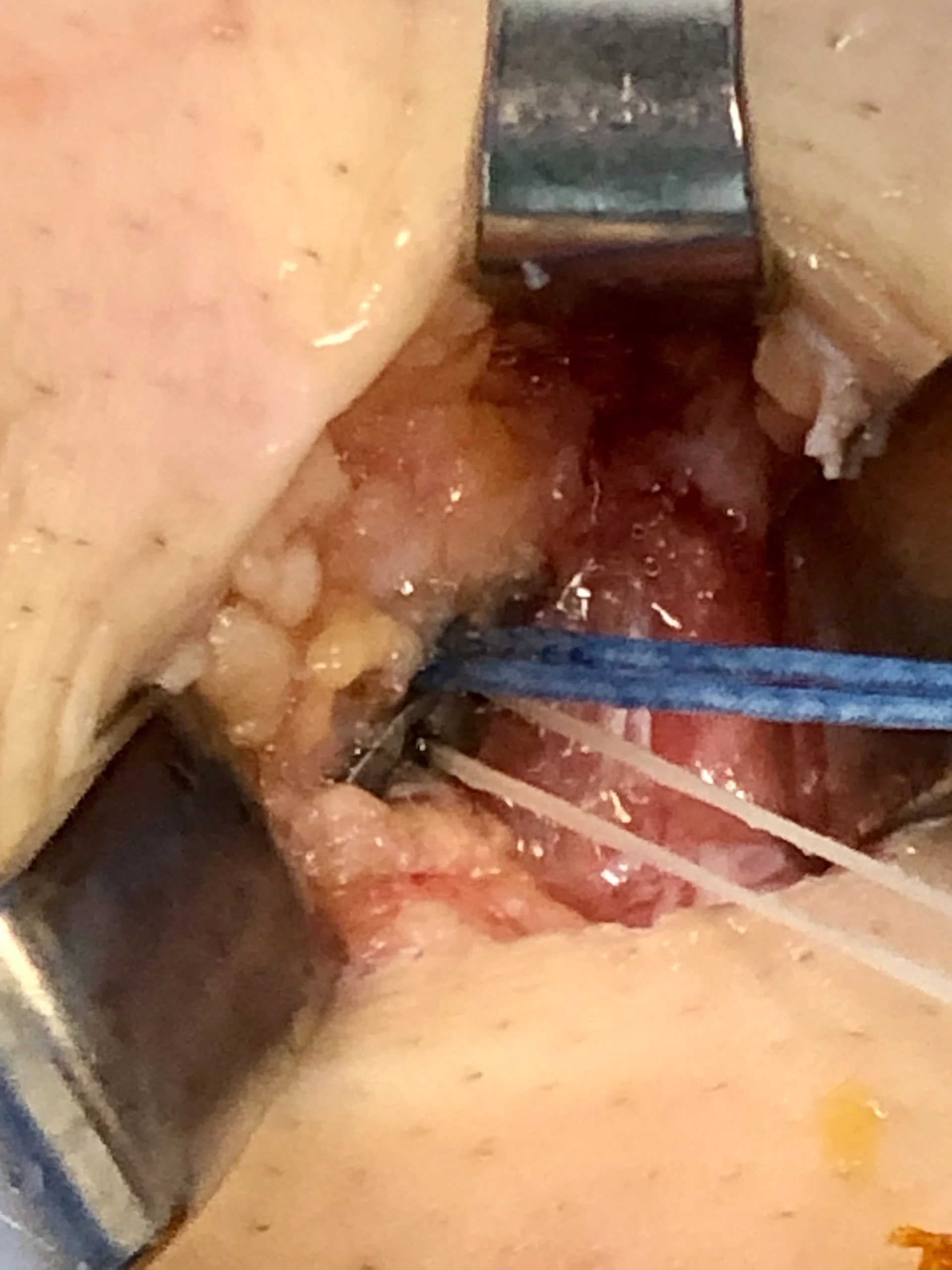
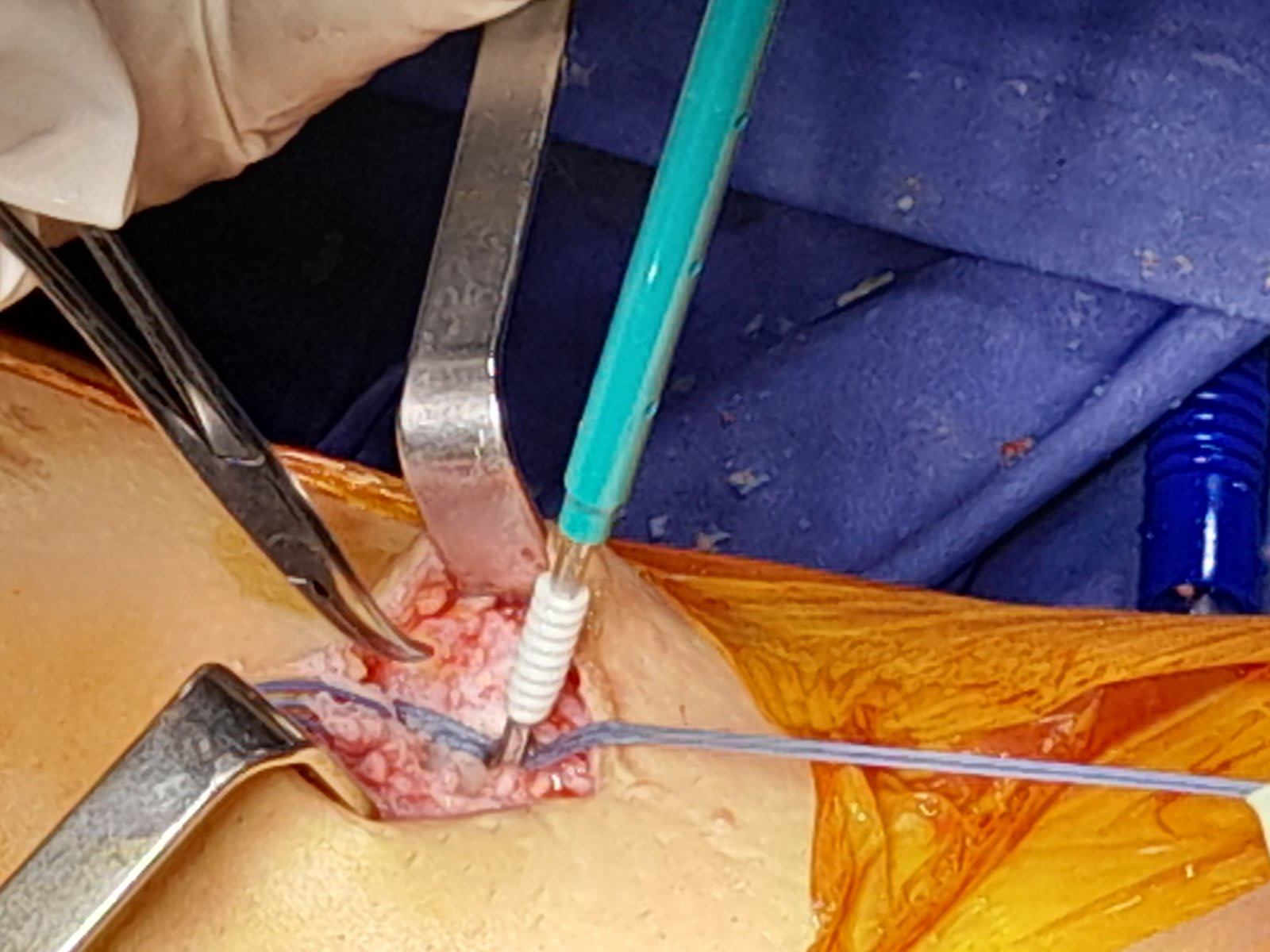
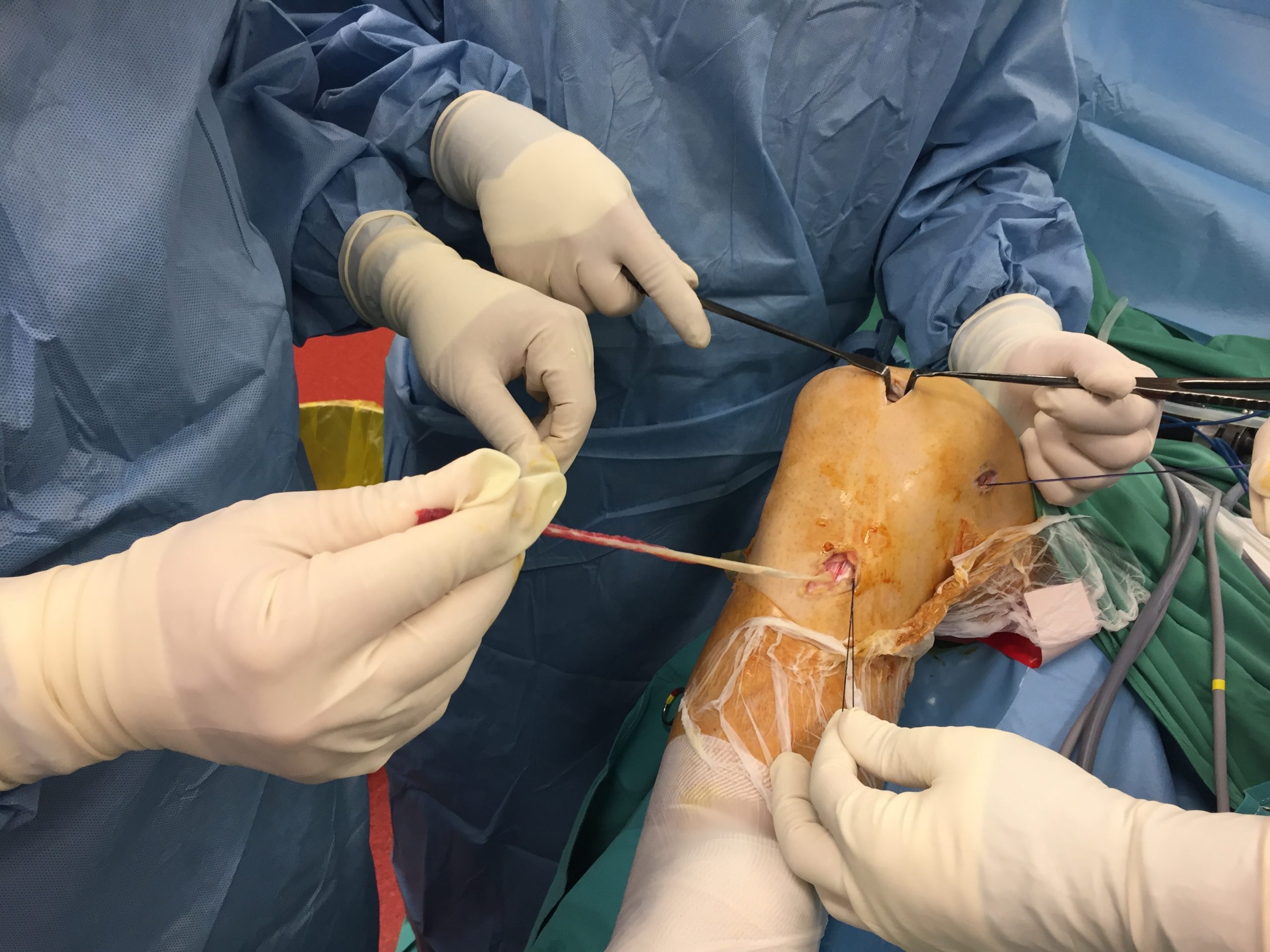
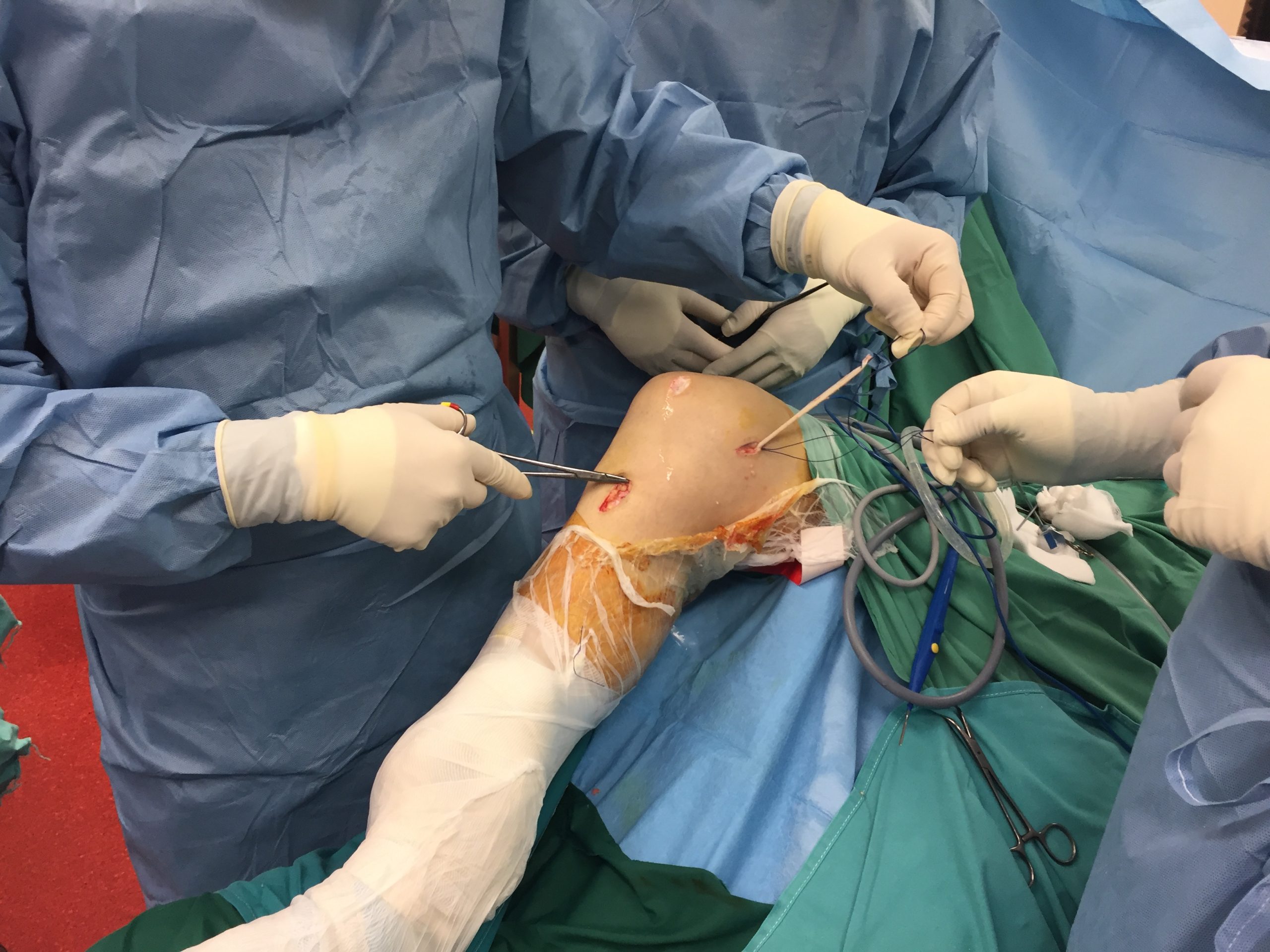
Il a pratiqué toutes les méthodes établies de reconstruction et de réparation du LCA, toutes les greffes et la quasi-totalité des meilleurs implants. Actuellement, il utilise soit les tendons ischio-jambiers , soit uniquement le tendon semi-tendineux avec la technique Arthrex « tout à l'intérieur ».

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Il utilise l'attelle interne Arthrex pour le renforcement, notamment chez les athlètes de haut niveau, les enfants, les femmes et pour les reprises chirurgicales.
{kind=link}
{kind=link}
Il utilise la technique de Lemaire modifiée de ténodèse extra-articulaire latérale comme complément à la reconstruction du LCA dans les cas à haut risque de déchirure du greffon, comme les cas de révision ou l'instabilité rotationnelle importante, et la technique de soutien interne ALL.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pathologie du cartilage
Le cartilage articulaire est le tissu lisse et blanc qui recouvre les extrémités des os, là où ils s'articulent pour former les articulations. Un cartilage sain facilite les mouvements. Il permet aux os de glisser les uns sur les autres avec un minimum de frottement. Le cartilage articulaire peut être endommagé par une blessure ou par l'usure normale.
Classification des lésions articulaires selon leur gravité
Grade | Outerbridge | Pont externe modifié | ICRS |
0 | cartilage normal | cartilage intact | cartilage intact |
je | Ramollissement et gonflement | Ramollissement ou formation de bulles chondrales avec surface intacte | Superficielles (indentation molle ou fissures et craquelures superficielles) |
II | Fragmentation et fissures dans une zone de diamètre inférieur à 0,5 pouce | Ulcération superficielle, fibrillation ou fissuration de moins de 50 % de la profondeur du cartilage | Lésion dont l'épaisseur est inférieure à la moitié de celle du cartilage articulaire |
III | Fragmentation et fissures dans une zone de plus de 0,5 pouce de diamètre | Ulcération profonde, fibrillation, fissuration ou lambeau chondral affectant plus de 50 % du cartilage sans exposition osseuse | Lésion dépassant la moitié de l'épaisseur du cartilage articulaire |
IV | Os sous-chondral exposé | Usure de pleine épaisseur avec os sous-chondral exposé | Lésion s'étendant à l'os sous-chondral |
De l'ICRS : Société internationale de réparation du cartilage
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Œdème de la moelle osseuse (contusion osseuse - lésion)
qu'une contusion osseuse survient lors de microfractures de la structure osseuse interne. Bien que ces microfractures n'affaiblissent pas significativement l'os, elles peuvent provoquer des saignements et une inflammation intra-osseuse. Ceci peut entraîner des douleurs et des symptômes similaires à ceux d'une contusion des tissus mous.
Des anomalies vasculaires, une diminution de la fibrinolyse (en particulier chez la femme enceinte) et une thromboembolie ont été proposées comme étiologies possibles, mais la cause exacte reste inconnue. En définitive, la douleur est probablement due à l'aggravation des faisceaux neurovasculaires au sein de la moelle osseuse, causée par une augmentation de la pression intra-osseuse due à l'accroissement du volume de liquide dans les espaces inter-médullaires.
Elle peut être provoquée par un traumatisme, l'arthrite, l'ostéoporose, des tumeursou des infections. Elle est fréquemment mal diagnostiquée car sa présentation clinique est très variable et non spécifique. De ce fait, elle peut être désignée par différents termes, notamment « ostéoporose transitoire », « ostéoporose migratoire régionale » et « algodystrophie ».
Le diagnostic repose sur l' IRM, qui révèle un hypersignal T2 de la moelle osseuse, une sensibilité aux fluides et une diminution du signal graisseux.
Le traitement vise à favoriser la guérison par les trois étapes suivantes : ostéoconduction,ostéoinductionetostéogenèse.
Le traitement conservateur comprend la mise en décharge (adaptation de l'activité), les médicaments anti-ostéoporotiques, les vitamines (bisphosphonates et supplémentation en vitamine D), la kinésithérapie spécifique et l'oxygénothérapie hyperbare.
En cas de contusion osseuse persistante, d'arthrose ou de nécrose avasculaire à un stade précoce, nous réalisons une décompression de la lésion et une injection directe de PRP et de cellules souches de concentré de moelle osseuse selon la technique de bioplastie intra-osseuse (IOBP/Biofiller) d'Arthrex. Nous utilisons également de la graisse microfragmentée injectée par voie intra-osseuse et intra-articulaire sous contrôle arthroscopique et fluoroscopique.
{kind=link}
{kind=link}
{kind=link}
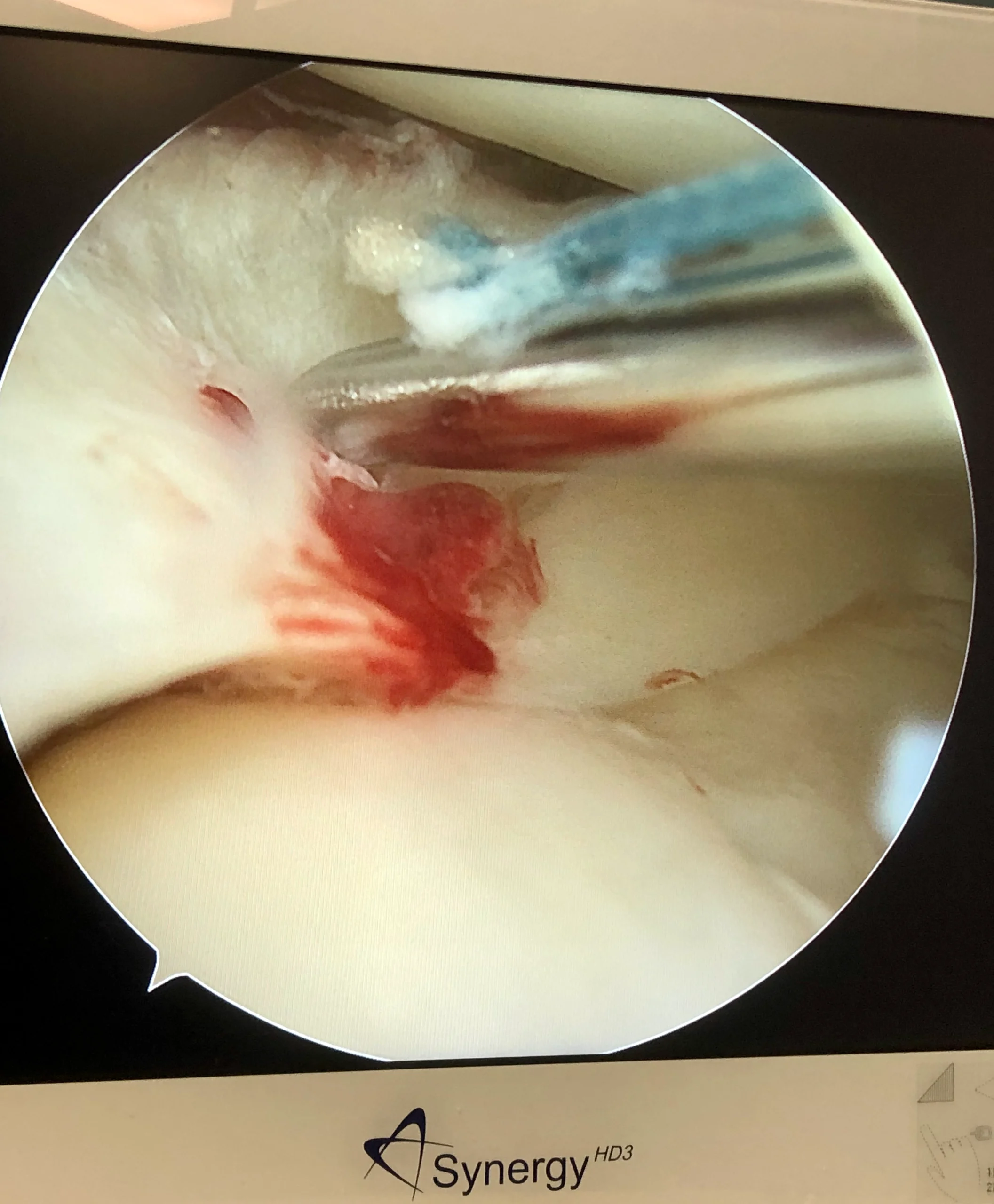
Luxation rotulienne - instabilité
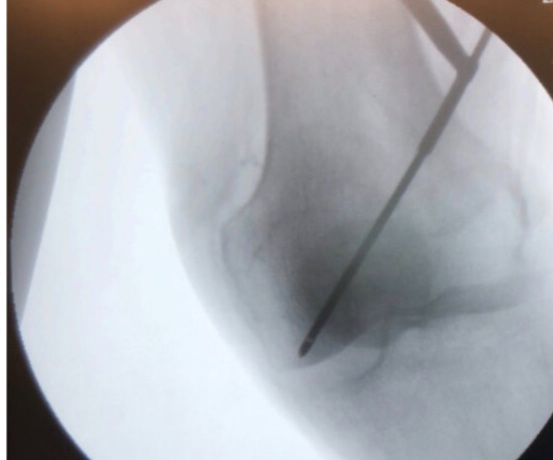
L'instabilité rotulienne est une affection caractérisée par des épisodes de subluxation ou de luxation de la rotule, consécutifs à un traumatisme, une laxité ligamentaire ou une augmentation de l'angle Q du genou. Le diagnostic est clinique en phase aiguë, en présence d'une luxation rotulienne associée à un épanchement articulaire traumatique , et en phase chronique, en présence d'une translation passive de la rotule et d'un signe J positif . L'IRM et le scanner sont des examens très utiles. Le traitement est non chirurgical, avec immobilisation par orthèse en cas de première luxation sans arrachement osseux ni présence de corps étrangers intra-articulaires . La prise en charge chirurgicale est indiquée en cas d' instabilité rotulienne chronique ou récidivante . Le traitement comprend le débridement arthroscopique (ablation du corps étranger) et la réparation, avec ou sans stabilisation . Indications : les fractures ostéochondrales déplacées ou la présence de corps étrangers intra-articulaires peuvent justifier un traitement chirurgical lors d'une première luxation . La reconstruction du ligament patello-fémoral médial (LPFM) peut être réalisée par autogreffe ou allogreffe . Indications: instabilité récidivante ou absence de malalignement sous-jacent significatif. Techniques: le gracilis ou le semi-tendineux sont couramment utilisés (plus résistants que le ligament patello-fémoral médial natif). L’origine fémorale peut être repérée de manière fiable par radiographie (point de Schottle). Un tunnel fémoral positionné trop proximalement entraîne une tension excessive du greffon (« haut et tendu »). Chez les patients pédiatriques, la fixation fémorale doit être réalisée plus antérieurement/distalement par rapport au point de Schottle. Une dysplasie trochléenne sévère est le facteur prédictif le plus important d’instabilité patello-fémorale résiduelle après reconstruction isolée du ligament patello-fémoral médial. La trochléoplastie est une intervention d’approfondissement trochléen, arthroscopique ou à ciel ouvert, pratiquée dans les cas sévères. Différents types d’ostéotomies , comme l’ostéotomie de Fulkerson et le transfert antérieur et médial de la tubérosité tibiale , peuvent être nécessaires
{kind=link}
{kind=link}
{kind=link}
{kind=link}
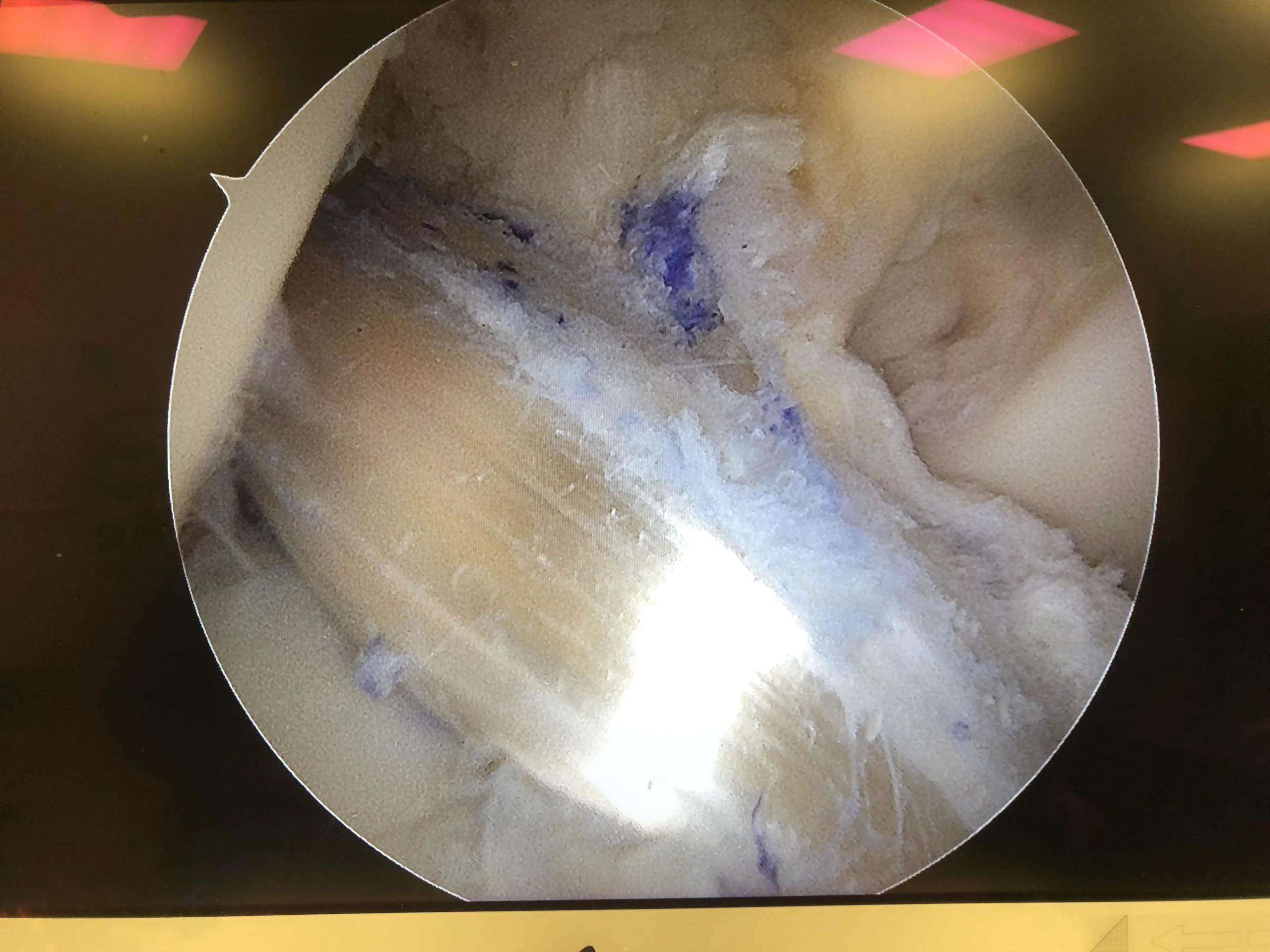
Ostéochondrite disséquante
- L'ostéochondrite disséquante est une lésion pathologique affectant le cartilage articulaire et l'os sous-chondral.
- Le diagnostic peut être établi par radiographie (vue de l'encoche), mais une IRM est généralement nécessaire pour déterminer la taille et la stabilité de la lésion, et pour documenter le degré de lésion cartilagineuse.
- Chez les enfants dont le cartilage de croissance est ouvert, le traitement peut être non chirurgical, avec une mise en charge partielle. Un traitement chirurgical peut être indiqué chez les patients plus âgés (cartilage de croissance fermé), en cas de lésions instables et chez les patients réfractaires au traitement conservateur.
| ||
|
| |
|
| |
|
| |
|
|
|
Traitement chirurgical selon le stade :
Forage sous-chondral avec broche de Kirschner ou foret/ fixation de la lésion instable / resurfaçage chondral.